Some people reading this are doing it in a dark room, one eye half-open, trying to decide whether the next canceled meeting, missed workout, or abandoned dinner plan means their migraines are getting worse again. You may already have a notebook full of triggers, a phone full of symptom apps, and a cabinet full of things that helped a little, then stopped helping enough.
That's the emotional context around microdosing for migraines. Many individuals don't arrive at this topic because it sounds trendy. They arrive because they're tired, curious, and willing to look at ideas that sit outside standard wellness advice.
Psilocybin microdosing has become one of those ideas. It sits in an awkward middle ground. It's not established migraine care. It's not a simple biohack. It's also not pure internet myth. There is early research worth understanding, but it's still early. That means the smartest way to approach it is with careful skepticism, clear tracking, and a strong safety filter.
This guide treats microdosing less like a shortcut and more like a personal research project. If you're going to explore it, the useful question isn't “Is this a cure?” It's “How would I observe this responsibly, without fooling myself or taking unnecessary risks?”
When Migraines Control Your Life
A familiar pattern goes like this. You wake up unsure whether the pressure behind your eye is just a bad morning or the start of a lost day. You scan your calendar first, not your messages, because the true question is whether you'll be able to function by noon.
Then the negotiation starts. Maybe more water. Maybe less screen time. Maybe coffee helps. Maybe coffee makes it worse. By afternoon, the migraine has turned the whole day into a math problem about light, sound, nausea, and disappointment.

The hidden burden
Migraines don't just hurt. They make ordinary planning feel unreliable. People stop trusting their own calendar. They keep backup plans for social events, work deadlines, and family time. Even a “good” day can feel fragile.
That's why alternative or emerging approaches get attention. If standard options haven't brought enough relief, people start looking at nutrition changes, sleep routines, supplements, meditation, and increasingly, psychedelic-adjacent wellness practices.
Migraines push people toward experimentation long before they push them toward confidence.
Why microdosing enters the conversation
Microdosing psilocybin often comes up in forums and conversations as something people hope might reduce migraine frequency rather than knock out a migraine in the moment. That distinction matters. Many readers hear “psilocybin” and assume this is about getting high or having a psychedelic experience. In the migraine conversation, that usually isn't the goal.
The more responsible framing is simple. This is an interesting but unproven option that some adults are curious about because early migraine research has shown signals worth paying attention to. Those signals don't erase the limits, legal issues, or safety concerns.
If you keep reading, keep that tone in mind. Curiosity is reasonable. Overconfidence isn't.
Understanding the Microdosing Concept
The word microdosing gets used loosely, which is one reason people get confused. In common use, it usually means taking a very small amount of a substance on a planned schedule with the aim of subtle effects, not a dramatic altered state.
A helpful analogy is a stereo knob. A full psychedelic dose is like turning the music up until it fills the room and demands your attention. A microdose is more like raising the background volume just enough that the atmosphere changes slightly, while you still go about your day.
What people usually mean by a microdose
In practical conversation, a microdose is meant to be sub-perceptual or near-sub-perceptual. In other words, the person isn't aiming for vivid sensory changes, a “trip,” or obvious intoxication. The intended effect, if there is one, is supposed to sit in the background.
That doesn't mean nothing happens. It means the hoped-for effect is subtle enough that many people need a journal to tell whether anything useful is changing.
Three ideas help separate microdosing from recreational use:
- Lower-intensity intent. The goal is usually everyday functioning, not a psychedelic session.
- Structured timing. People often use planned intervals instead of spontaneous use.
- Observation over sensation. The main question becomes whether patterns shift over time, especially migraine frequency, severity, recovery, mood, or tolerance to triggers.
Why the term causes confusion
One major source of confusion is that “microdosing” often gets mixed together with any low dose. Those aren't always the same thing. Some research on migraine has used low doses that may still be better described as clinically low exposure rather than a classic community-style microdose.
That difference matters because readers can mistakenly assume every positive study proves common self-directed microdosing works the same way. It doesn't. Research terms, community habits, and product labeling don't always line up neatly.
Practical rule: If you can't clearly describe what you mean by “microdose,” you're not ready to evaluate whether it's helping.
What microdosing is not
It's not a guaranteed treatment. It's not automatically safer because the amount is smaller. And it's not something you can judge by one unusually good day.
A lot of wellness trends survive because people remember the standout experience and forget the baseline. That's especially risky with migraines, where symptoms naturally rise and fall. Without structured observation, it's easy to credit a substance for changes that might have happened anyway.
What the Research Says About Psilocybin and Migraines
A person with frequent migraines can read one hopeful headline and start filling in the rest of the story. Relief. Fewer lost days. Maybe a way out. The research does not support that kind of shortcut yet. What it does offer is an early signal that deserves careful attention.
The strongest migraine-specific evidence so far comes from a very small pilot trial that tested a single low dose of psilocybin in people with migraine. Researchers saw a reduction in migraine burden compared with placebo, and that result was strong enough to keep scientific interest alive. Small pilot studies work like a flashlight, not a floodlight. They can show where something may be worth investigating, but they do not show the full room.
That distinction matters for anyone considering microdosing as a personal experiment. A positive pilot study does not mean community-style microdosing has been proven to prevent migraines. It means one controlled study found a signal under specific conditions.
Researchers also take the topic seriously because migraine prevention is often built on pattern changes over time rather than immediate pain relief. If you want background on the broader brain science behind that interest, this overview of how psilocybin affects brain signaling gives helpful context.
The wider headache literature adds both interest and caution. Reviews of psychedelic research in headache disorders suggest that some people report benefit, but the studies vary a lot in dose, design, diagnosis, and follow-up. That makes the findings hard to compare directly. It is a bit like trying to judge a recipe when each cook used different ingredients, different ovens, and different timing.
Dose is one of the biggest sources of confusion. Some reports include low-dose use, some include clearly psychedelic doses, and some rely on retrospective self-report rather than tightly controlled migraine trials. That is why a reader should be careful with summaries that compress all of this into one simple takeaway. “Psilocybin helped headaches” is too vague to guide a responsible decision.
Safety signals also deserve equal space in the conversation. Smaller amounts are not automatically free of side effects, and higher amounts are not automatically better. Across the broader headache literature, researchers have described temporary increases in anxiety, pain, and cardiovascular measures in some participants. Early research can point to promise and risk at the same time.
The practical takeaway is modest but useful. Psilocybin has enough early evidence in migraine to justify more study. It does not have enough evidence to act like settled medical guidance.
For readers who still want to explore the idea, the most responsible frame is personal research, not self-certainty. Treat each observation like a data point, not a verdict. If the pattern is real, careful tracking should make it clearer over time. If it is not, good records help prevent wishful thinking from writing the conclusion for you.
Potential Pathways for Migraine Prevention
Researchers are interested in psilocybin for migraine because the biology makes enough sense to justify testing it. That's different from saying the mechanism is fully proven. It isn't.
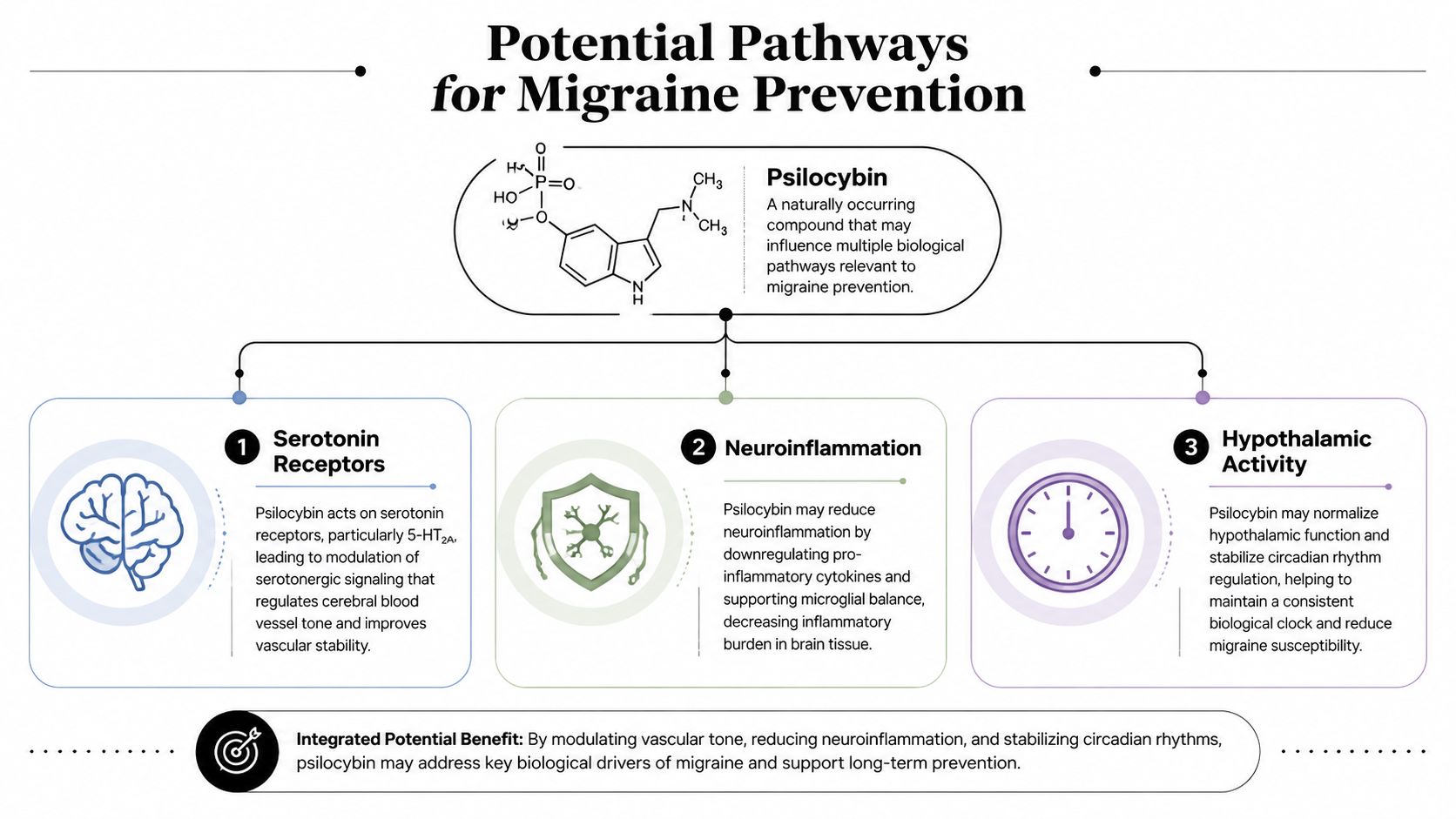
One useful way to think about migraine prevention is to picture the brain as a control room that sometimes becomes too reactive. The goal of a preventive treatment isn't usually to silence pain instantly. It's to make the control room less likely to spiral into an attack.
Serotonin signaling
Psilocybin interacts with the brain's serotonin system, especially receptors often discussed in psychedelic research. Migraine researchers care about this because serotonin pathways are already closely tied to migraine biology.
Think of serotonin signaling as part of the brain's traffic-light system. If the timing gets off, vascular and nerve-related processes may become more unstable. A substance that changes signaling in that system could, in theory, alter how often the migraine process gets triggered.
A placebo-controlled crossover study of 10 chronic migraine patients found that a single oral dose of synthetic psilocybin at 0.143 mg/kg (about 10 mg for a 65-kg adult) produced a statistically significant reduction in migraine frequency per week (P = .004), along with lower pain severity, functional impairment, and weekly abortive-medication use versus placebo, as summarized in WebMD's review of psilocybin migraine research.
Inflammation and brain reactivity
Another theory involves neuroinflammation and overactive signaling networks. The idea isn't that psilocybin works like a standard painkiller. It may act more like a system reset, nudging some circuits away from a chronically reactive state.
That may help explain why people talk about prevention rather than rescue. If a treatment changes the threshold for attacks, you might notice fewer bad days over time rather than dramatic same-hour relief.
A short visual helps make those pathways easier to picture.
Why dose still matters
Many people overreach at this stage. If a pathway is promising, they assume more exposure must create more benefit. Migraine data doesn't support that simple story. The target seems to be neuromodulation, not maximum intensity.
A preventive strategy is more like tuning an instrument than hitting a mute button.
That's why cautious readers should think in terms of threshold effects, tolerability, and pattern changes. Not dramatic sensations.
Common Protocols and The Importance of Tracking
People who explore microdosing usually don't dose randomly. They follow a repeatable schedule so they can compare days with exposure and days without it. The schedule itself isn't magic. Its real value is that it creates cleaner observations.
Common schedules people talk about
Below are examples often discussed in microdosing communities. They are not recommendations and they aren't validated migraine protocols. They show how people try to impose structure on something that can otherwise become vague.
| Example Microdosing Schedules (Not a Recommendation) | Schedule | Typical Rationale |
|---|---|---|
| Fadiman-style approach | One day on, two days off | Creates space between doses and may make it easier to notice patterns |
| Every-other-day approach | Dose, skip, dose, skip | Simpler routine for people who want a steady comparison rhythm |
| Short cycle with reset | Several scheduled dosing days followed by a longer break | Used by people trying to reduce habit-like use and reassess baseline |
| Stamets-style stack discussion | Often described as psilocybin paired with other ingredients on a planned cycle | Framed by users as a broader wellness routine rather than psilocybin alone |
If you want to understand how adults commonly describe these approaches in practical terms, this guide to microdosing with magic mushrooms is one example of how the conversation is framed outside formal clinical literature.
The journal matters more than the protocol
A journal is the actual tool. Without one, your brain will cherry-pick memorable days and ignore the ordinary ones.
Track the same variables every time. Keep it boring. Boring data is useful data.
A solid migraine-focused log often includes:
- Dose and timing. Record the amount, the form, and the time you took it.
- Migraine activity. Note whether a migraine happened, how long it lasted, and whether it felt different from your usual pattern.
- Pain and function. Track pain level, but also whether you could work, drive, read, exercise, or tolerate screens.
- Mood and energy. These can shift independently of migraine pain and may color your interpretation.
- Possible triggers. Sleep disruption, skipped meals, stress, alcohol, hormonal shifts, weather changes, and unusual caffeine intake belong in the notes.
- Side effects. Anxiety, restlessness, nausea, agitation, or anything new should be logged, even if it seems minor.
How to avoid fooling yourself
Use a before-and-after framework. Spend time tracking your baseline pattern before making changes, then compare that pattern with your tracking during any experimental period. The less dramatic your method feels, the more trustworthy your conclusion will be.
You can also create simple decision rules in advance:
- Stop if side effects become concerning.
- Stop if your migraine pattern clearly worsens.
- Reassess if you can't tell whether anything is happening except on “interesting” days.
- Don't stack major lifestyle changes at the same time if your goal is to learn what's doing what.
If someone wants to approach microdosing for migraines responsibly, this is the center of gravity. Not the schedule. Not the hype. The record.
Navigating Safety Risks and Legal Realities
A person with frequent migraines can get desperate fast. After enough canceled plans, missed work, and dark-room afternoons, a small dose can start to sound like a small risk. That is often where people make preventable mistakes.

Psilocybin is not just a migraine idea. It is a psychoactive substance with mental, physical, and legal consequences attached to it. If you treat microdosing as a personal research project, safety checks belong in the same notebook as symptom notes. A scientist would not run an experiment without checking the hazards first. The same logic applies here.
Risk starts before the first dose
The main question is not only, “Could this help?” It is also, “What makes me a poor candidate to test this on myself?”
Some situations raise the stakes:
- Psychiatric vulnerability. A personal or family history of psychosis, mania, or severe mood instability can make psychedelic exposure much riskier.
- Medication interactions. Psilocybin does not exist in isolation. Antidepressants, mood stabilizers, stimulants, and other drugs can complicate the picture. This guide on psilocybin interactions with antidepressants and related medications gives a useful overview of why this deserves careful review.
- Cardiovascular concerns. Any substance that may shift stress response, heart rate, or blood pressure deserves extra caution if you already have heart or circulation issues.
- Complicated migraine history. Rapidly changing symptoms, severe neurological features, or uncertainty about your diagnosis call for medical input before adding another variable.
A simple rule helps here. If your health history is complicated enough that you would struggle to summarize it clearly to a clinician, self-experimentation is probably not the right starting point.
Small doses can still create real problems
People sometimes hear “microdose” and assume “barely active.” That is not a safe assumption. Even low doses can produce anxiety, restlessness, nausea, agitation, or a strange increase in body awareness. For someone already prone to panic, sensory sensitivity, or fear around an approaching migraine, those effects can muddy the picture fast.
That matters for practical reasons. If a dose makes you feel keyed up, distracted, or perceptually off, driving, working, or making treatment decisions may become harder, not easier.
Legal status is not simple
Local policy, state policy, and federal law are not interchangeable. A city may reduce enforcement priority, yet possession can still remain illegal under broader law. Social media often flattens those distinctions into “it's basically legal,” which is a poor standard for risk assessment.
Readers in Michigan should be especially careful with this point. Local shifts may change day-to-day enforcement in some places, but they do not erase the larger legal framework. Before obtaining, possessing, or using psilocybin, know the rules that apply where you live.
A clinician can help you pressure-test the plan
You do not need to ask a doctor for philosophical approval. A better conversation is concrete and specific.
Explain your migraine goal. List all your medications, supplements, and other substances. Ask about mental health risks, cardiovascular concerns, and signs that would mean stop immediately. If you present the idea as a structured experiment instead of a last-ditch impulse, the conversation is often more useful.
Caution is not overreaction here. It is part of doing the experiment responsibly.
A Template for Cautious Personal Exploration
If you decide to explore microdosing for migraines, treat your notes like field research. Keep entries short, consistent, and honest. Don't write what you hope is happening. Write what happened.
| Simple Microdosing Journal Template | Dose (mg or g) | Migraine Today? (Yes/No) | Pain (1-10) | Mood (1-10) | Notes (Triggers, Side Effects, etc.) |
|---|---|---|---|---|---|
You can copy that into a notes app, spreadsheet, or paper log. The format matters less than consistency.
It's also worth remembering that psilocybin doesn't need to carry this whole conversation. Many people also explore non-psychedelic migraine supports such as magnesium, CoQ10, mindfulness practices, sleep regularity, hydration, and trigger tracking. For some, those belong alongside experimentation. For others, they're the safer place to start.
Start low. Go slowly. Stop if your data or your body tells you this isn't helping.
If you're an adult in Southeast Michigan looking for practical education around psilocybin products, Metro Mush publishes guides on topics like microdosing and offers product information for local consumers in the Detroit and Ann Arbor areas. Use that kind of resource as a starting point for informed questions, not as a substitute for careful self-monitoring or medical judgment.