You might be in a very specific spot right now. Your antidepressant helps you function, or at least keeps the floor from dropping out. At the same time, you've read about psilocybin, heard friends talk about shrooms, or seen headlines about depression research and wondered whether this could help you too.
That curiosity makes sense.
A 2021 Imperial College London clinical trial on psilocybin for depression found that remission rates were twice as high in the psilocybin group compared with the escitalopram group, and people in the psilocybin group reported greater reductions in anxiety and increased feelings of wellbeing. That kind of result naturally raises a difficult question for anyone already taking medication. What happens if both are in the picture at once?
The short answer is that shrooms and antidepressants can interact in more than one way. Sometimes the psychedelic effects are weakened. Sometimes the safety picture depends heavily on the medication class. Sometimes the bigger danger isn't the combination itself, but stopping an antidepressant too quickly in order to try psilocybin.
Many people find themselves stuck at this point. They do not want a lecture. They want practical guidance that takes their real situation seriously.
That's what this article is for. Not a green light. Not a blanket prohibition. A cautious, harm-reduction guide for the medicated-but-curious person who wants to understand the tradeoffs before doing anything risky.
Navigating Psychedelic Curiosity While on Antidepressants
A common scenario goes like this. Someone has been on an SSRI for months or years. Maybe it helps with panic, depression, or obsessive spirals, but it also feels emotionally flattening. Then they start hearing that psilocybin may help people reconnect with emotion, meaning, and motivation. The question isn't abstract anymore. It's personal.
That question deserves a careful answer because both substances are tied to mental health, but they don't operate in the same way. One is a daily medication meant to stabilize symptoms over time. The other is a fast-acting psychedelic compound that can produce intense changes in perception, emotion, and insight. Putting them together isn't as simple as combining two things that both affect mood.
People also get mixed messages. One source says never combine them. Another says it only weakens the trip. Another focuses on cutting-edge clinical studies and makes it sound like antidepressants no longer matter. None of those one-line answers are enough.
Practical rule: If you're considering shrooms and antidepressants together, the first question isn't "Will I trip?" It's "What am I taking, why am I taking it, and what happens if I change that plan?"
That shift matters. For some people, the biggest risk is a bad interaction. For others, it's destabilizing their mental health by changing medication too fast. For others still, it's expecting a therapeutic result from a blunted or unpredictable experience.
The safest approach starts with understanding the mechanism, then the medication class, then the actual risks. Once those pieces are clear, you can make better decisions with a prescriber instead of guessing from internet anecdotes.
How Shrooms and Antidepressants Affect Brain Chemistry
Your brain's serotonin system is often described in overly technical language, but the basic idea is simple. The system functions as a network of locks, keys, and traffic signals. Different chemicals can open certain locks, block certain signals, or change how responsive the system is over time.
Psilocybin is converted in the body to psilocin, which mainly acts on the 5-HT2A receptor. That's one of the main receptor sites linked to the psychedelic experience. When people talk about altered perception, unusual thought patterns, emotional intensity, or a sense that their usual mental filters have loosened, that receptor is a big part of the story.

For a deeper plain-English primer, this overview of psilocybin effects on the brain is a useful companion to the interaction questions covered here.
What antidepressants do differently
Antidepressants don't all work the same way. The most common ones, SSRIs and SNRIs, don't create a psychedelic effect. Instead, they change serotonin signaling in a steadier, background way. You can think of them less like a sudden key turning a lock, and more like a long-term adjustment to the whole control panel.
Over time, that can matter because the brain adapts. Receptors may become less responsive to certain signals, even if serotonin activity is increased overall. This is one reason a person can be taking a serotonin-related medication and still have a weaker response to psilocybin.
Why the interaction feels confusing
Many readers get tripped up by this logic. They assume, "If both affect serotonin, wouldn't combining them make the effects stronger?" Not necessarily.
A better analogy is a dimmer switch. Psilocybin tries to light up a specific circuit. Some antidepressants change the wiring enough that the signal doesn't land with the same intensity. That can mean fewer visuals, less emotional opening, or a generally muted experience.
Two substances can affect the same system and still push in different directions.
That's also why anecdotes vary so much. One person reports almost no psychedelic effects. Another reports a subtle but meaningful shift. A third has a strong experience anyway. The medication class, the individual brain, the dose, and the broader mental health context all matter.
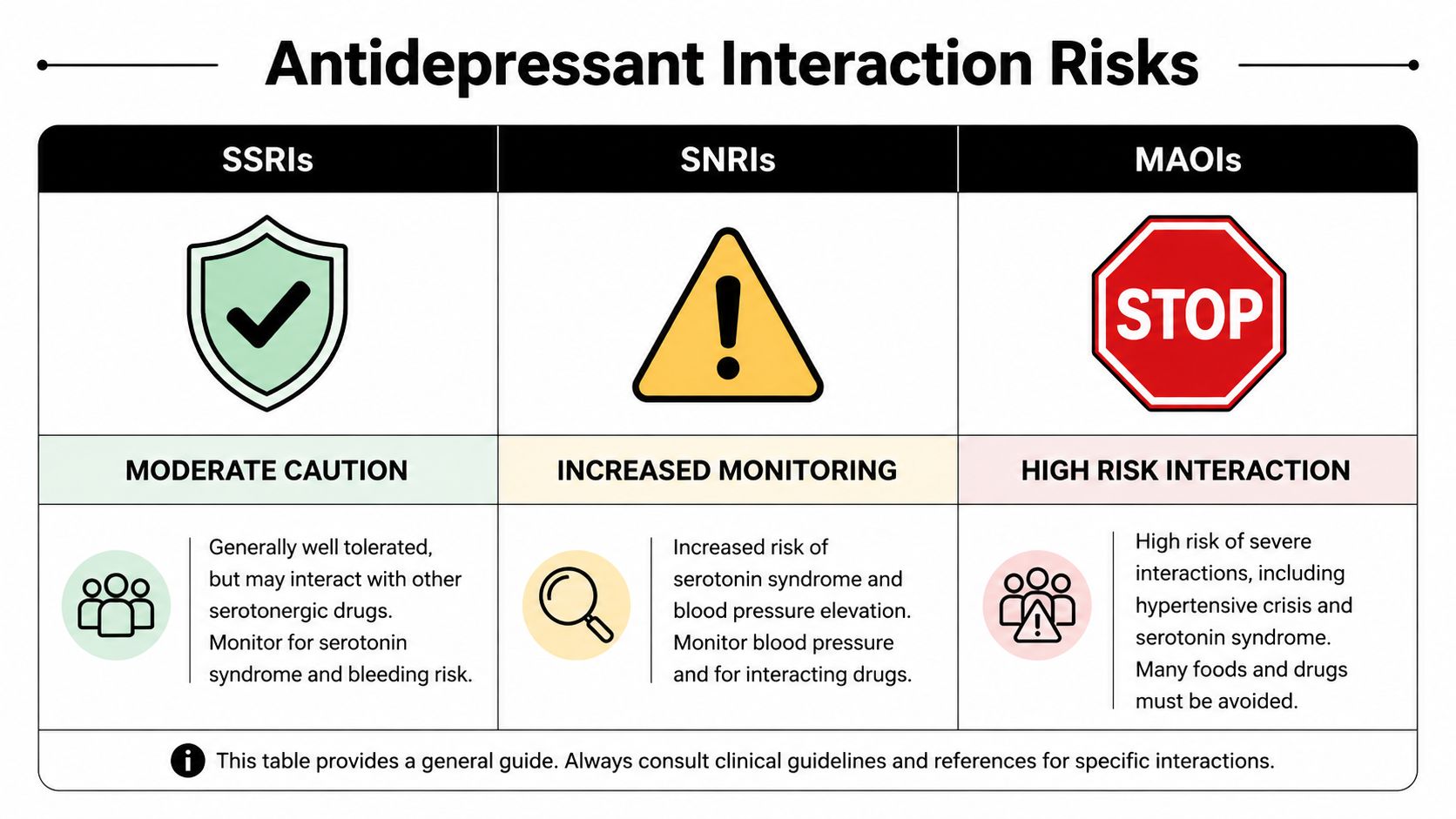
Interaction Risks by Antidepressant Class
If you're trying to evaluate shrooms and antidepressants realistically, medication class matters more than the broad label "antidepressant." Some combinations are mostly associated with blunted effects. Others raise more serious safety concerns.
If you want context on why clinical programs handle these combinations so carefully, this explanation of what psychedelic therapy involves helps show why medication review is such a major part of screening.
The comparison that matters most
A retrospective survey on antidepressants and psilocybin found that SSRIs diminished psychedelic effects in 47% of users, SNRIs did so in 55%, and bupropion in 29%. The same research linked this blunting effect to antidepressant-related changes in the 5-HT2A receptors that psilocybin targets, according to the Johns Hopkins publication on attenuation during and after SSRI or SNRI use.
Here is the practical version of that information:
| Antidepressant Class | Common Examples | Interaction with Psilocybin | Primary Risk |
|---|---|---|---|
| SSRIs | sertraline, fluoxetine, escitalopram, paroxetine, citalopram | Often associated with a weaker or flatter psychedelic experience | Reduced effect, harder-to-predict response |
| SNRIs | venlafaxine, duloxetine | Similar to SSRIs, often with blunting and a need for extra caution | Reduced effect, monitoring concerns |
| MAOIs | phenelzine, tranylcypromine | Higher-risk interaction profile | Potentially dangerous serotonin-related or cardiovascular complications |
| TCAs | amitriptyline, nortriptyline | Less clear, varies by drug and person | Uncertain interaction, medical review needed |
| Atypicals | bupropion, mirtazapine and others | Not one uniform category. Effects depend on mechanism | Medication-specific concerns rather than one single rule |
SSRIs and SNRIs
For many people, this is the category that matters most. The typical issue isn't a dramatic medical emergency. It's disappointment, unpredictability, or a misleadingly weak experience.
Someone might take a dose expecting a full psychedelic effect and instead get something partial. That can create a bad feedback loop. They may think the material is weak, then take more, not realizing the medication is changing the response rather than "blocking" it in a clean way.
This is also why advice from a friend can be dangerous. If your friend isn't on an SSRI, their experience doesn't map cleanly onto yours.
MAOIs
This is the class that deserves the most caution. A lot of online discussion lumps all antidepressants together, but MAOIs are not in the same practical category as SSRIs.
With MAOIs, the concern goes beyond a muted trip. The interaction profile is more serious, and the possibility of a dangerous adverse event rises enough that this combination shouldn't be treated casually.
If you're on an MAOI, this is not a self-experiment situation.
Bupropion and other atypicals
People often ask whether all antidepressants weaken psilocybin in the same way. The answer is no.
The same retrospective survey found that bupropion weakened effects in 29% of cases, which was lower than the rates reported for SSRIs and SNRIs in that dataset. That doesn't make it automatically safe or simple, but it does suggest that non-serotonergic antidepressants can behave differently.
The catch is that "atypical antidepressant" is a broad bucket. Bupropion is not mirtazapine, and mirtazapine is not a TCA. Once you leave the SSRI and SNRI categories, one-size-fits-all advice gets weaker fast.
A better way to think about your medication
Instead of asking "Can I mix shrooms and antidepressants?" ask these questions:
What exact medication am I on
The generic name matters more than the brand reputation.What class is it in
SSRI, SNRI, MAOI, TCA, or atypical changes the conversation.What is my real goal
Are you seeking symptom relief, curiosity, emotional access, or a recreational experience?What happens if I stop or reduce this medication
For many people, that risk is more immediate than the psilocybin interaction itself.
Understanding Blunted Effects and Serotonin Syndrome
Two concerns dominate this topic. The first is blunted effects. The second is serotonin syndrome, which gets talked about constantly but often without enough nuance.
Blunted effects are common enough to plan around
When people on SSRIs or SNRIs say shrooms "didn't work," they often don't mean nothing happened at all. They may mean the experience felt thinner, less visual, less immersive, or less emotionally open than expected.
That matters because a weaker subjective experience can lead to poor decisions. A person might redose too soon. They might mix substances. They might assume more is always the answer. In reality, the medication may be altering the receptor response in a way that makes the experience less straightforward, not merely underdosed.
There is another layer here. A muted psychedelic experience doesn't necessarily mean there is zero therapeutic effect. A recent clinical paper noted that a 25 mg dose of synthetic psilocybin given to patients on stable SSRIs showed comparable antidepressant efficacy to antidepressant-free trials, with only mild side effects and no serotonin syndrome in that study, according to the Frontiers report on psilocybin with concomitant SSRIs.
That doesn't mean home use is equivalent to clinical care. It does mean the story is more complicated than "SSRIs cancel psilocybin."
Serotonin syndrome deserves respect, not panic
Serotonin syndrome is a potentially serious toxic state linked to excess serotonergic activity. The reason people worry about it here is obvious. Both psilocybin and many antidepressants touch the serotonin system.
However, the actual situation is more specific than the internet usually suggests. A 2024 review of 18 studies concluded that combining classic psychedelics with antidepressants was "generally safe and tolerable" with no significant increase in adverse events, according to the review of antidepressant and psychedelic coadministration. That same review also noted a case report of hypertensive emergency when psilocybin was combined with an MAOI and an antidepressant, which points to where the sharper danger may lie.
What this means in plain language
For many individuals asking about shrooms and antidepressants, the likely issue is not instant catastrophe. It's altered effects and an uncertain response.
For a smaller group, especially people taking MAOIs or multiple interacting drugs, the concern becomes more medically serious. This is one reason polypharmacy changes the conversation. Once several medications are in play, guessing gets riskier.
A low-drama answer is usually the honest one. The combination may be tolerated in some situations, but "tolerated" is not the same as predictable, optimal, or appropriate for self-directed use.
A Practical Harm Reduction Framework
If you're considering shrooms and antidepressants, use a framework that assumes your brain chemistry is not a blank slate. That's not a reason for shame. It's a reason to slow down.

Start with the non-negotiable step
Talk to the clinician who prescribes your medication, or another qualified medical professional who understands both antidepressants and psychedelics. The goal isn't just permission. It's to review your diagnosis, medication class, any history of mania or psychosis, and the risk of changing treatment.
This matters especially because research indicates the blunting effect from SSRIs can persist for up to 3 months after discontinuation, and some users report weakened effects even two years after stopping antidepressants, as noted in the PubMed summary of antidepressant-related attenuation findings. There is no universally agreed washout timeline.
Build your safety plan before deciding anything
A practical plan should include:
Medication review
Know the exact drug, dose, class, and how long you've been taking it.No abrupt stopping
Antidepressant withdrawal can be destabilizing on its own. A taper, if medically appropriate, should be supervised.Set and setting
If someone proceeds despite the cautions, mindset and environment matter. A chaotic apartment, unresolved conflict, or an impulsive late-night decision can make a hard situation worse.A sober support person
Someone trusted should know what you've taken, what medications you're on, and when to seek help.
For general trip safety basics, this guide on how to avoid bad trips is useful, especially for people who are focused on emotional safety as much as physical safety.
Don't treat blunting like a dosing challenge
Harm reduction often fails in such situations. A person hears that SSRIs may weaken effects, so they conclude the answer is to take more psilocybin.
That logic can backfire. Blunting does not create a neat mathematical formula. The interaction may alter the quality of the experience, not just the intensity. Redosing or escalating can create confusion and risk without giving you the result you expected.
The safest mindset is to treat uncertainty itself as a risk factor.
If your situation is medically complex, or if your antidepressant is the reason you're stable enough to function, caution is not overkill. It's the adult move.
Recognizing Emergency Signs and Getting Help
If someone has taken shrooms while on antidepressants and starts showing signs of a severe reaction, don't wait for certainty. Act.
Potential warning signs include:
- Agitation or severe restlessness
- Confusion or sudden disorientation
- Rapid heart rate
- High blood pressure
- Dilated pupils
- Heavy sweating
- Muscle rigidity or unusual stiffness
- Tremor or shaking
- High fever
- Seizure-like activity
These symptoms can overlap with panic, intoxication, or other medical problems, which is exactly why guessing is dangerous. If the symptoms are intense, escalating, or involve fever, rigidity, cardiovascular distress, or altered consciousness, call 911 or go to the nearest emergency room.
If you're the sober support person, bring or photograph the medication bottles if possible. Tell responders what was taken, when it was taken, and what prescription medications are involved. Clear information helps medical staff respond faster.
A person having a frightening psychedelic experience without clear physical danger may need calm reassurance, reduced stimulation, and monitoring. A person showing signs of a toxic or cardiovascular reaction needs emergency care.
The Future of Combining Psychedelics and Antidepressants
The science here is moving away from simplistic slogans. "Never mix them" is too broad. "They're fine together" is also too broad. What research is starting to suggest is more interesting and more demanding. Different drugs, doses, and clinical settings may produce very different outcomes.

One of the most notable developments is that a recent study found a 25 mg dose of synthetic psilocybin in patients on stable SSRIs showed comparable antidepressant efficacy to antidepressant-free trials, with mild side effects and no cases of serotonin syndrome. That finding doesn't erase the concerns covered above. It does suggest that future treatment models may not require every patient to fully discontinue medication before participating in carefully designed care.
Why clinical settings may look different from personal use
A clinic can control screening, dose, monitoring, and follow-up. It can exclude high-risk combinations. It can respond if symptoms worsen. Personal use doesn't offer those safeguards.
That's why research can point toward a future therapeutic pathway without translating into a casual recommendation for self-experimentation. Context changes everything.
For readers who want a broader sense of how this field is evolving, this video offers added perspective.
The most responsible takeaway is also the least flashy. If you're exploring shrooms and antidepressants, don't rely on myths, bravado, or trial-and-error. Use medical guidance, respect the differences between antidepressant classes, and treat uncertainty as something to manage rather than ignore.
If you're an adult in Southeast Michigan looking for psilocybin products and want a retailer that takes education, accessibility, and local convenience seriously, explore Metro Mush. You can browse dried mushrooms, chocolates, drinks, and low-dose options while staying grounded in a harm-reduction mindset: know what you're taking, know your medications, and when in doubt, slow down and ask better questions first.