You’ve probably seen this topic arrive from three directions at once. A news headline says psychedelics may help depression or PTSD. A friend tells you about a life-changing mushroom experience. A podcast swings between neuroscience and spiritual language so quickly that it’s hard to tell what’s medicine, what’s marketing, and what’s myth.
That confusion makes sense.
When people ask what is psychedelic therapy, they’re often asking several questions at once. Is this real medicine? Is it just taking mushrooms and hoping for insight? Who is it for? Is it legal? Is it safe? And if someone isn’t in a formal clinic, what does “responsible use” even mean?
Psychedelic-assisted therapy sits at the intersection of psychiatry, neuroscience, ethics, and culture. It’s promising. It’s also easy to misunderstand. The clearest way to approach it is to separate the structured medical model from other forms of psychedelic use, then look at each with honesty.
The Growing Buzz Around Psychedelic Healing
The renewed interest in psychedelic healing isn’t coming from one small corner of wellness culture. It’s showing up in hospitals, universities, policy debates, veterans’ communities, and ordinary family conversations. That matters because the subject has moved beyond fringe curiosity.
A recent UC Berkeley poll found that 61% of American registered voters support legalized regulated therapeutic access to psychedelics, with especially high support for terminal illness at 80% and veterans at 69%, according to the UC Berkeley Center for the Science of Psychedelics survey summary. Those numbers don’t mean everyone agrees on how psychedelics should be used. They do show that many people now see therapeutic use as a serious medical question.
Why people feel both hopeful and skeptical
Part of the buzz comes from dissatisfaction with existing mental health treatments. Some people don’t respond well enough to standard antidepressants. Others feel stuck in long-standing trauma patterns even after years of therapy. When they hear that a different approach may help, their attention sharpens fast.
At the same time, psychedelics carry baggage. Some people associate them with the counterculture. Others have heard exaggerated claims that make them sound like a cure-all. Neither extreme is helpful.
Psychedelic therapy makes the most sense when you hold two ideas at once. It may be a breakthrough for some people, and it still requires careful screening, skilled support, and realistic expectations.
What this conversation is really about
The public conversation often gets muddled because it combines very different things under one label:
- Clinical treatment: structured care with screening, preparation, monitored sessions, and follow-up.
- Personal exploration: self-directed use outside formal medical systems.
- Commercial hype: products, branding, and bold promises that may outpace evidence.
- Cultural and spiritual practice: traditions that don’t fit neatly into a medical model.
If you separate those paths, the subject becomes much easier to understand. That’s where a grounded explanation begins.
Defining Psychedelic Assisted Therapy
Psychedelic-assisted therapy is not just taking a psychedelic. It’s a structured therapeutic protocol in which a psychedelic substance is used as one part of a broader treatment process guided by trained professionals.
The simplest way to understand it is this. The psychedelic is the tool. The therapy is the method that makes the tool useful.
A hammer can build a house or break a window. A surgical instrument can heal only in skilled hands and in the right setting. In the same way, a psychedelic compound may open a powerful mental and emotional state, but the healing work depends on preparation, support, and what happens afterward.
The medicine is not the whole treatment
People often assume the substance itself does all the work. That’s one of the biggest points of confusion.
In psychedelic-assisted therapy, the drug creates a temporary window of openness. During that window, a person may feel less stuck in familiar thoughts, more emotionally connected, or more able to revisit painful material without their usual defenses locking everything down. But insight alone doesn’t guarantee change.
Therapy gives the experience structure. It helps a person prepare for what may come up, stay oriented during the session, and translate what they learn into daily life.
What makes it different from recreational use
The difference isn’t just legality. It’s purpose, design, and support.
In a therapeutic setting, the process usually includes:
- Screening: clinicians look for reasons the treatment may not be appropriate, including certain psychiatric or medical concerns.
- Preparation: the patient and therapist build trust, review history, discuss fears, and clarify intentions.
- Monitored dosing: the session takes place in a controlled environment designed to reduce unnecessary stress.
- Integration: afterward, the patient works with a therapist to make sense of the experience and apply it.
Core idea: The psychedelic may help loosen rigid patterns. The therapy helps a person rebuild in a healthier direction.
A better way to think about the word therapy
The word “therapy” here doesn’t mean passive relaxation. It means active psychological work.
Some people cry. Some revisit old trauma. Some experience awe, grief, relief, or confusion. Some have insights that feel highly meaningful in the moment but need careful unpacking later. A good therapist helps distinguish between a moving experience and a useful one.
That’s why the phrase what is psychedelic therapy is best answered as a process, not a product. It’s a clinical framework built around a powerful altered state, with the goal of lasting mental and emotional change.
How Psychedelics Change the Brain
A person can spend years caught in the same mental loop. The thoughts may change on the surface, but the track underneath stays familiar: fear, self-criticism, avoidance, hopelessness. One reason psychedelic-assisted therapy has drawn so much medical interest is that it may briefly loosen those well-worn tracks, giving therapy a better chance to help.
A simple comparison helps here. A sled path after many runs becomes fast and automatic. The brain works in a similar way. Repeated thoughts and reactions become easier to follow over time. That efficiency can support healthy habits, but it can also reinforce depression, trauma responses, and compulsive patterns.
Receptors, plasticity, and a temporary period of flexibility
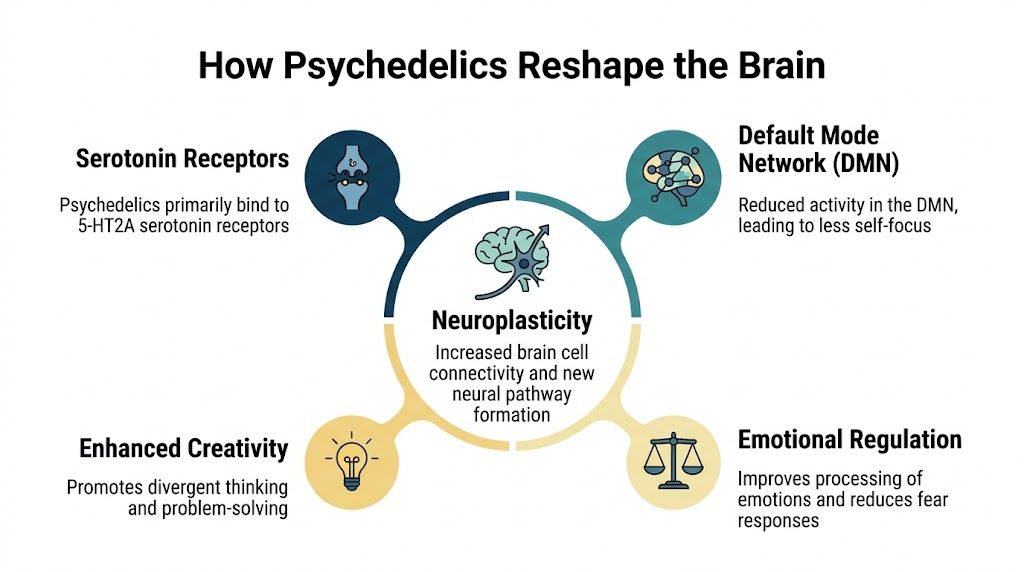
Classic psychedelics such as psilocybin mainly act on 5-HT2A serotonin receptors. Research published by Nature Reviews Neuroscience describes these drugs as producing a temporary brain state associated with altered perception, changes in self-processing, and greater neural flexibility.
That last phrase can sound abstract, so it helps to translate it. Neural flexibility means the brain may become more able, for a limited period, to form new connections and respond differently than usual. It is less like permanently rewiring a house and more like opening a window while repairs are being made.
For a closer explanation of these mechanisms, this guide to psilocybin effects on the brain connects the neuroscience to what people may notice during an experience.
The Default Mode Network, in plain English
Another term people often hear is the Default Mode Network, or DMN. This network is linked to self-focused thinking, autobiographical reflection, and the inner story a person tells about who they are. Researchers at Johns Hopkins Center for Psychedelic and Consciousness Research describe psychedelics as affecting brain systems involved in perception, mood, and sense of self, which helps explain why the experience can feel so psychologically significant.
In plain language, the DMN helps maintain the brain’s “usual story.” That story can be useful. It gives continuity and identity. But when someone is depressed or traumatized, the story can become painfully rigid: “I always fail.” “I am broken.” “Nothing will change.”
Psychedelic states may temporarily reduce the grip of that rigid self-narration. A useful comparison is a choir in which one section has been singing too loudly for a long time. If that section quiets down for a while, other voices become easier to hear.
Why this matters in therapy, and why context matters so much
A more flexible brain state does not equal healing by itself. The setting, the support, and the psychological work shape what happens during that opening. This is the distinction many people miss when they ask what is psychedelic therapy.
In psychedelic-assisted therapy, clinicians use that temporary period of flexibility as part of a structured treatment process. The medicine may make a person less defended, more emotionally open, or able to view painful memories from a different angle. The therapy helps turn that moment into learning that lasts.
Outside a clinical framework, the same temporary openness can become confusing, destabilizing, or unfocused. That does not mean every non-clinical experience is meaningless. It means the outcome depends much more on preparation, safety, support, and what happens afterward. The brain may be more open to change for a period of time. What gets reinforced during that period matters.
A Look at Common Psychedelic Modalities
“Psychedelic therapy” is a broad label. It covers several substances with different effects, different research histories, and different levels of medical acceptance. Lumping them together creates confusion fast.
Some compounds are considered classic psychedelics, such as psilocybin and LSD. Some, like MDMA, are often discussed alongside psychedelics in therapy even though the subjective experience is different. Ketamine also gets included in the public conversation because it’s already used clinically for mental health care, though it works through a different pharmacologic pathway. Ayahuasca adds another layer because it often appears in ceremonial rather than standard medical settings.
Comparison of Psychedelic Therapy Modalities
| Substance | Primary Therapeutic Target | Typical Experience | Legal/Medical Status (2026) |
|---|---|---|---|
| Psilocybin | Depression, end-of-life distress, substance use questions in research | Often introspective, emotionally vivid, sensory changes, shifts in self-perspective | Strong research interest and therapeutic discussion, with access varying by jurisdiction |
| MDMA | PTSD | Often more empathic, less defended, emotionally connected, trauma material may feel more approachable | Advanced clinical interest, with legal access dependent on jurisdiction and medical pathway |
| Ketamine | Depression and related symptoms in clinical settings | Can feel dissociative, dreamlike, or perspective-shifting | Available through established medical pathways in licensed settings |
| LSD | Depression, anxiety, and other indications in research contexts | Long-lasting classic psychedelic effects, intense shifts in perception and meaning | Primarily research or non-clinical contexts depending on jurisdiction |
| Ayahuasca | Spiritual, trauma, and personal-growth contexts, sometimes discussed alongside therapy | Often intense, symbolic, emotional, physically demanding, usually group or ceremonial | Generally outside standard medical care, with legal status varying widely |
Psilocybin and why it gets so much attention
Psilocybin, the psychoactive compound associated with “magic mushrooms,” is probably the substance widely implied when one asks what psychedelic therapy is. It has become a leading focus in depression research and in public discussions about mushroom-based treatment.
The experience often includes strong shifts in emotion, autobiographical memory, meaning, and self-perception. Some people feel connected and expansive. Others move through grief, fear, or buried material before reaching clarity. In therapeutic use, those reactions are held inside a structured container rather than treated like random side effects.
MDMA and trauma work
MDMA tends to be described differently because the experience often feels less like a classic trip and more like a state of emotional safety, openness, and reduced fear. That profile is one reason it has drawn major attention in PTSD treatment.
People with trauma often know exactly what happened to them, but their nervous system reacts as if the danger is still present. A treatment that helps lower fear while preserving emotional access may create a very different kind of therapeutic opportunity.
MDMA-assisted therapy is often discussed with psychedelic medicine because it can transform the emotional conditions under which therapy happens, even though many people experience it differently from psilocybin or LSD.
Ketamine LSD and ayahuasca
Ketamine is important because it gives many people their first real-world example of legally available altered-state treatment in a clinic. A person may not call it psychedelic, but in practice it often introduces the same core idea: an unusual state of consciousness can be therapeutically useful when handled carefully.
LSD has a long history in psychedelic research and culture. It remains influential conceptually, but in mainstream clinical discussion it’s less central than psilocybin or MDMA.
Ayahuasca occupies a distinct space. People often encounter it through retreat or ceremonial settings rather than standardized mental health clinics. That doesn’t make it meaningless. It does mean the support model, expectations, and risk profile may differ substantially from formal psychedelic-assisted therapy.
A careful reader should notice the key dividing line here. It isn’t merely which substance is “best.” It’s whether the context around the substance is medical, ceremonial, peer-supported, or self-directed. That context changes almost everything.
Clinical Evidence for Psychedelic Healing
A person who has spent years trying antidepressants or trauma therapy may hear about psychedelic treatment and wonder whether this is medicine, hype, or a little of both. The answer starts with the quality of the evidence. What has drawn hospitals, medical schools, and regulators into this field is not curiosity alone. It is the fact that some carefully run studies have produced results that are difficult for psychiatry to ignore.
That said, the evidence supports a very specific model of care. Researchers are studying psychedelic-assisted therapy, not casual psychedelic use, not retreat marketing, and not unsupervised self-experimentation. That distinction matters because the treatment is more like a surgical procedure than a supplement. The drug is only one part of the protocol. Screening, preparation, therapeutic support, and follow-up shape the outcome.
Depression research
One of the studies that changed the public conversation came from Johns Hopkins. In a randomized clinical trial of adults with major depressive disorder, psilocybin sessions combined with supportive psychotherapy were associated with large and rapid reductions in depression symptoms, according to Johns Hopkins Medicine’s summary of the trial. In a follow-up report, the same research group found that some participants maintained benefits at 12 months, which suggests the treatment may work on a different timeline from daily medications for some people, as reported by Johns Hopkins Medicine.
That does not mean psilocybin is a universal answer for depression. It means researchers have documented meaningful improvement under controlled conditions, with trained support and careful patient selection.
PTSD research
The clearest evidence for MDMA-assisted therapy has focused on PTSD. A phase 3 study published in Nature Medicine found that participants receiving MDMA-assisted therapy had greater reductions in PTSD symptoms than those in the therapy-plus-placebo group, with a substantial share no longer meeting diagnostic criteria after treatment, according to the published trial report.
Why does that result stand out? PTSD often locks people into fear, avoidance, and hypervigilance. In that state, therapy can feel like trying to repair an engine while it is still racing. MDMA appears to change the emotional conditions enough for some patients to stay engaged with painful material instead of shutting down or becoming overwhelmed.
What the evidence does and does not show
The pattern across the strongest studies is fairly consistent. Benefit appears most convincing in structured treatment programs for depression and PTSD, especially when the altered state is embedded in psychotherapy rather than treated as a stand-alone event. Researchers are also studying addiction, end-of-life distress, and other conditions, but those areas are still developing.
The limit is just as important as the promise. Results from a clinic or trial do not automatically transfer to a retreat, a ceremonial setting, or a person using psychedelics alone at home. Different setting, different screening, different support, different risk.
A useful rule is simple. The closer the situation is to the protocol used in the study, the more reasonable it is to compare the outcome. The farther it moves from that protocol, the weaker that comparison becomes.
The Three Stages of a Therapy Journey
A person may spend weeks preparing for a single treatment day, then spend weeks afterward making sense of it. That pacing surprises people who picture psychedelic therapy as one dramatic event. In clinical care, it works more like surgery followed by rehabilitation. The medicine may create the opening, but the surrounding care helps determine whether that opening leads to insight, relief, or confusion.
The three stages are preparation, the dosing session, and integration. Together, they show the difference between psychedelic-assisted therapy and other forms of psychedelic use. A retreat, a ceremony, or self-directed use may include some of these elements, but medical protocols build the whole process on screening, consent, therapeutic support, and follow-up.

Preparation before anything happens
Preparation gives the experience a container. Without it, a person can enter an unusually open and vulnerable state without a clear plan for what to do if fear, grief, or disorientation shows up.
This stage usually includes several practical tasks. The therapist reviews mental health history, current symptoms, medications, and personal goals. The patient learns what the altered state can feel like, how the room will be set up, what kinds of support are available, and what limits apply around touch and boundaries.
A simple comparison helps here. Preparation works like drawing a map before entering unfamiliar terrain. The map does not remove uncertainty, but it lowers the chance that surprise turns into panic.
Common preparation topics include:
- Intention setting: a direction for the work, such as grief, trauma, self-criticism, or a repeating relationship pattern
- Practical agreements: who will be present, how the session will unfold, and how support will be offered
- Coping plans: what to do if the experience becomes intense, confusing, or emotionally raw
- Logistics after the session: transportation, rest, and who can offer grounded support at home
This is also the stage where people often realize that interest is not the same as readiness. Someone who is curious about psilocybin may still need careful screening, or may decide that a legal educational resource about magic mushrooms in Michigan fits their needs better than pursuing treatment right away.
The dosing session itself
The dosing day is structured to reduce distraction and help the person stay with inner experience. In many therapy models, the room is calm, the pace is slow, and clinicians remain present throughout the session. Eyeshades and music are often used to support inward focus, and physical contact is limited to situations where consent has been discussed clearly in advance.
That setup can seem unusual at first. It helps to compare it to lowering the lights in a theater so your attention turns to the screen. The point is not sensory novelty. The point is to make it easier to notice emotions, memories, body sensations, and patterns of thought without getting pulled outward every few minutes.
Here’s a short visual overview of how the process is commonly described in practice.
The therapists are not there to direct a performance. They are there to maintain safety, offer reassurance, and help the person stay oriented if the experience becomes overwhelming. That is one of the clearest differences between psychedelic-assisted therapy and unsupervised use. The medicine may be similar. The level of preparation, monitoring, and clinical responsibility is not.
Integration is where change gets anchored
Integration turns an intense experience into something a person can use in daily life. A session may bring up a powerful memory, a burst of self-compassion, or a painful realization about a relationship. None of that automatically becomes change.
Integration sessions help the person sort signal from noise. Some impressions will feel meaningful and still need testing against ordinary life. Others may be emotionally true but incomplete. A good therapist helps translate insight into specific next steps, such as a boundary, a conversation, a grief ritual, a change in routine, or a different way of responding during stress.
Three questions often guide this stage:
- What happened beneath the most dramatic moments?
- Which insights still feel true after sleep, reflection, and discussion?
- What action belongs to this experience, if any?
That final point matters. Psychedelic-assisted therapy is not defined by having unusual perceptions. It is defined by a structured process that helps a patient prepare safely, experience the session with support, and then make careful meaning from it afterward.
Navigating Safety Legal and Ethical Issues
A person can hear that psychedelics are helping with depression or trauma, find a retreat or underground guide online, and assume the main question is whether the substance works. Safety asks a different question first: under what conditions, with which people, and with what safeguards?
That distinction matters because psychedelic-assisted therapy is a structured care model, not merely psychedelic use with a helpful conversation around it. In legitimate care, screening, informed consent, crisis planning, follow-up, and professional accountability are part of the treatment itself.
Some people should not proceed, or should only proceed after careful medical review. A history of psychosis, bipolar-spectrum conditions, certain cardiovascular concerns, or medication interactions can change the risk profile in a meaningful way. Antidepressant changes also require caution. Stopping or tapering psychiatric medication without medical supervision can create its own problems, even before a psychedelic session enters the picture.
Safety includes the room, the relationship, and the rules
Medical screening is only one layer.
Psychological and ethical safety shape what the experience becomes. An altered state can lower defenses and increase suggestibility. That is useful in therapy only when the setting is trustworthy, boundaries are clear, and the clinician treats consent as an ongoing process rather than a form signed at intake.
A good provider should be able to explain basic questions in plain language. How are medical and psychiatric risks screened? What happens if fear, confusion, or traumatic material surfaces? Are there policies around touch, privacy, and emergency response? Who handles integration if the session brings up issues that continue for days or weeks?
Culture belongs in this conversation too. Care can follow a formal protocol and still miss the person in front of it. Language about healing, surrender, spirituality, family, race, or trauma does not mean the same thing in every community. Ethical care accounts for that difference before the session, during the session, and after it.
Researchers writing about equitable psychedelic care make a similar point in this analysis of psychedelic care for underserved communities. Access by itself does not create safety or trust. People also need preparation, support, and a treatment frame that fits their lived reality.
Legal access and clinical care are different tracks
The legal situation is layered. Federal law, state policy, local decriminalization efforts, clinical trials, ketamine practice, and future licensing programs do not all mean the same thing, and they do not offer the same protections.
A useful comparison is the difference between an open road and a regulated transportation system. One means people may be traveling. The other means there are licenses, inspections, training standards, and procedures when something goes wrong.
That is why decriminalization should not be confused with therapy. Reduced penalties may change law enforcement priorities. They do not automatically create clinician training, product testing, adverse event reporting, or standards for who is qualified to guide vulnerable patients. For readers trying to sort out that local policy picture, this guide to magic mushrooms in Michigan explains how local enforcement shifts differ from legality and from formal medical treatment.
Questions that protect patients
If you are evaluating a clinic, retreat, or guide, direct questions can reveal a lot:
- How do you screen for psychiatric, medical, and medication-related risks?
- What license, clinical training, or supervision do you work under?
- How do you handle consent, boundaries, and physical contact?
- What is your plan if a session becomes overwhelming or medically concerning?
- How is integration provided after the experience?
- How do you adapt care for a person's cultural background, trauma history, and belief system?
Clear answers suggest structure. Evasive answers suggest risk.
The core ethical point is simple. Psychedelic-assisted therapy should be judged like any other serious health intervention. The questions are not only whether a substance can help, but whether the setting is lawful, the provider is accountable, and the process protects the person at their most vulnerable.
How to Find Legitimate Care and Information
If you’re interested in psychedelic therapy, the safest first step is to get clear about which path you’re considering. People often mix together medical treatment, research participation, retreat experiences, local access, and self-directed use as if they’re interchangeable. They aren’t.
The main paths people take
Some people pursue the most structured route available: clinical research or licensed medical treatment. Clinical trials generally offer the highest level of screening, monitoring, and protocol. In some regions, ketamine clinics also provide a legal, established model for altered-state treatment under medical supervision.
Others are watching for future changes in state-regulated or federally approved pathways for psilocybin or MDMA. This area is constantly changing, and it’s worth checking the current rules where you live rather than relying on social media summaries.
Then there’s the path many people already take. They explore psychedelics outside formal therapy.
If the setting is not clinical
It is important to be honest. Many adults use psychedelics in non-clinical contexts, whether through community networks, private circles, retreat spaces, or products they obtain directly. That reality exists whether the medical system is ready for it or not.
For those situations, harm reduction becomes the practical framework. Research and clinical commentary emphasize that mindset, or “set,” and environment, or “setting,” profoundly influence outcomes, and that integrating challenging experiences can become a catalyst for growth, as discussed in this balanced overview of psychedelic therapy risks and integration.
A few grounded principles help:
- Know your context: why you’re doing this, what emotional state you’re in, and whether now is a stable time.
- Choose your setting carefully: privacy, calm, and trusted company matter.
- Plan support ahead of time: don’t wait until after a difficult experience to decide who you’ll talk to.
- Respect integration: journaling, therapy, peer support, or community discussion can help translate experience into something useful.
- Be skeptical of hype: “natural” doesn’t mean risk-free, and profound doesn’t always mean beneficial.
How to evaluate information sources
A trustworthy source usually sounds more measured than magical. It acknowledges uncertainty. It screens for risks. It distinguishes between evidence from trials and stories from personal use. It doesn’t promise enlightenment, a cure, or guaranteed transformation.
If you’re trying to sort through local options and practical realities, it also helps to compare information from clinical organizations, peer-reviewed discussions, and local educational resources rather than relying on one voice alone. Readers looking at the broader local market can browse mushroom suppliers near me as part of understanding what kinds of non-clinical access exist, while still keeping a clear boundary between product availability and formal therapy.
The most important takeaway is simple. Psychedelic-assisted therapy is a specific, structured treatment model. It is not the same thing as all psychedelic use. But if someone isn’t in a clinic, that doesn’t mean the conversation ends. It means safety, preparation, and integration become even more important.
If you’re an adult in Southeast Michigan exploring psilocybin products and want a clearer view of local options, Metro Mush offers a Detroit and Ann Arbor focused menu with dried mushrooms, chocolates, and drinks, along with practical ordering information and community updates. Whether you’re cautious, experienced, or just starting to understand the options available, take the same approach this guide recommends. Stay informed, move deliberately, and treat psychedelic use with respect.