You might be on Zoloft, feeling stable enough that you're finally able to think about other options for healing. Then you start hearing about psilocybin. Friends talk about insight, relief, or emotional breakthroughs. Clinical research gets shared all over social media. Naturally, one question shows up fast: what happens with Zoloft and mushrooms?
Most articles answer that question too bluntly. They either say “never mix them” and stop there, or they drift into speculation. The more useful reality is messier. For many people, the biggest issue isn't a dramatic toxic reaction. It's that the mushrooms may feel weaker, flatter, or oddly muted.
That matters because it changes the decision people face. The dilemma often isn't just “Is this dangerous?” It's “Will anything happen at all, and is it worth changing my medication to find out?” That second question can lead people toward risky choices, especially abrupt SSRI stopping.
The Growing Question About Zoloft and Psilocybin
Zoloft, or sertraline, is an SSRI. Psilocybin is being studied for depression and other mental health conditions, but those two facts don't automatically mean they work well together. In practice, many people encounter difficulty. They aren't trying to party recklessly. They're trying to make sense of two different approaches to mental health that both touch the serotonin system.
The cultural shift around psilocybin is part of why this question keeps coming up. A major Imperial College London trial compared psilocybin with the SSRI escitalopram and found that 70% of participants in the psilocybin group achieved at least a 50% reduction in depression scores, while 48% in the escitalopram group did, and remission at week 6 was 57% versus 28%. At the same time, the primary between-group comparison was not statistically significant, and the researchers said larger trials are still needed, as reported by Imperial College London's summary of the 2021 trial.
Why this gets confusing fast
That study is easy to misunderstand. It doesn't show that taking an SSRI and psilocybin together is proven safe, proven effective, or clinically standard. If anything, it highlights the opposite point. Most rigorous studies look at psilocybin as an alternative to SSRIs, not as something routinely combined with them.
The intersection of “Zoloft and mushrooms” presents a question that modern science still hasn't answered cleanly.
What makes this topic hard: people often borrow hope from psilocybin research without noticing that many studies don't test the exact situation they're in, namely taking sertraline and using mushrooms at the same time.
That doesn't mean your question is unreasonable. It means you need a more careful answer than a simple warning label.
How Zoloft and Mushrooms Compete in Your Brain
The simplest way to understand Zoloft and mushrooms is to think about serotonin signaling like a busy venue with limited access points.
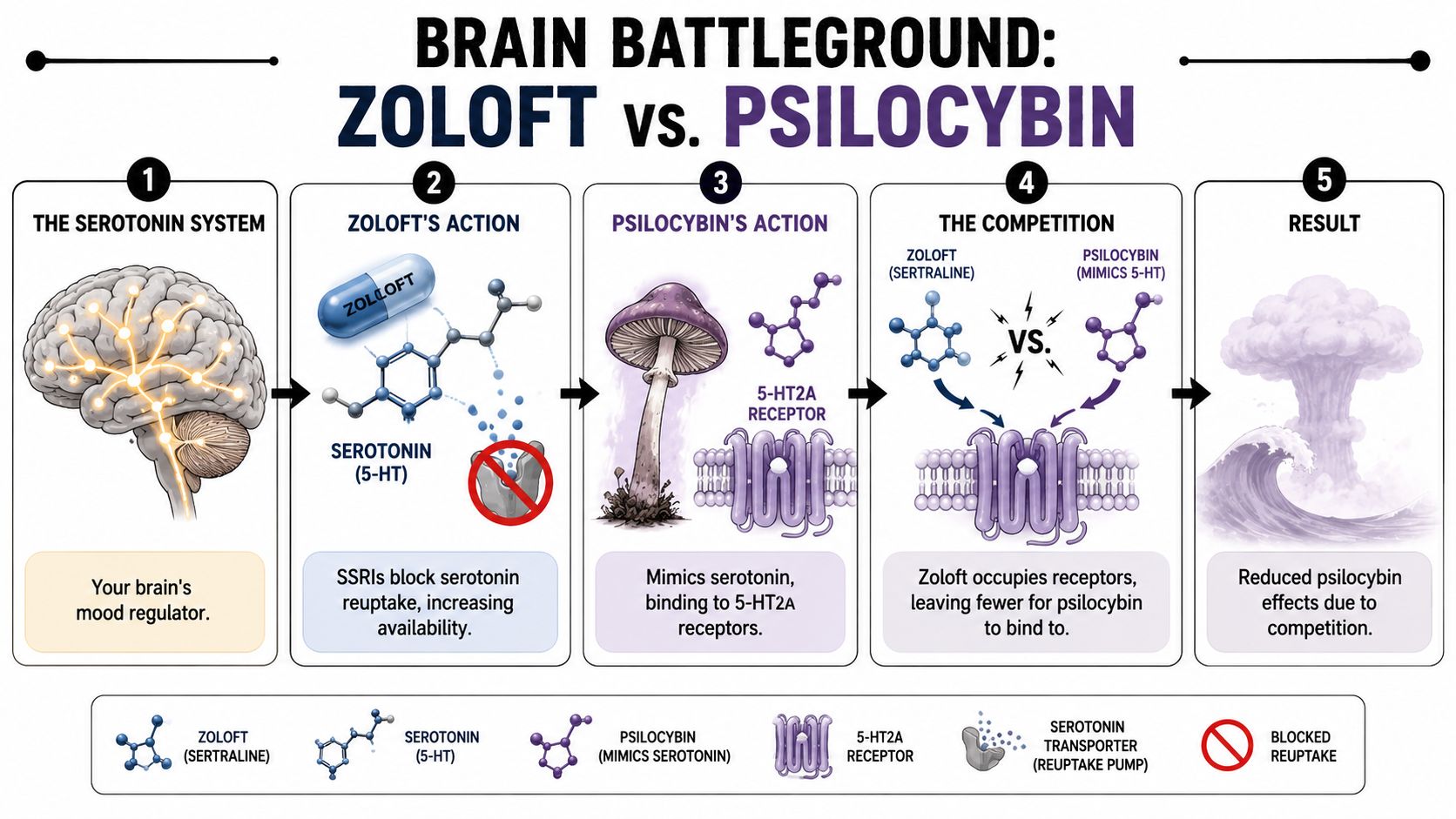
Your brain uses serotonin as one of its chemical messengers. Zoloft changes that system by blocking serotonin reuptake, which leaves more serotonin active in the synapse over time. Psilocybin, once converted into psilocin, creates its psychedelic effects largely by acting at serotonin receptors, especially 5-HT2A.
The concert hall analogy
Think of the serotonin system as a concert hall.
- Serotonin is the regular crowd. It shows up every day.
- Zoloft keeps more of that crowd inside the hall for longer.
- Psilocin is a special guest performer trying to create a noticeable effect through a particular set of seats and speakers.
If serotonin signaling remains high over time, the brain doesn't just sit there passively. It adapts. Receptors can become less responsive or less available. So when psilocin arrives, it may not hit with the same force it would in someone who isn't taking an SSRI.
That helps explain why many people describe the combination as underwhelming rather than explosive.
Why this doesn't feel intuitive
A lot of people assume the logic should be simple. If both substances involve serotonin, then adding them together should create a stronger experience. Pharmacology often doesn't work that way. More overlap doesn't always mean more intensity. Sometimes it means interference.
One substance can change the terrain the other depends on.
If you want a broader primer on how psilocybin changes perception and brain signaling, this overview of psilocybin effects on the brain is a useful companion to the interaction question.
What users often notice
The most common reports are less cinematic than people expect:
- Softer visuals: Colors and patterning may be weaker than expected.
- Reduced emotional depth: The “opening up” people describe with psilocybin can feel partially blocked.
- A ceiling effect: Taking more doesn't necessarily produce the breakthrough someone was hoping for.
- An uneven experience: Some body sensations may still appear, while insight or immersion feels muted.
You can think of SSRIs less like a dangerous collision and more like a volume limiter. That's not a perfect analogy, but it fits many real-world reports better than scare stories do.
The Blunted Trip Why Effects Are Often Weaker
When people ask about Zoloft and mushrooms, the most evidence-based answer isn't “you'll definitely have a medical emergency.” It's that the trip may be weaker than expected.
A 2023 survey study published on PubMed looked at 611 self-reports of taking mushrooms while on antidepressants. Among people on SSRIs, 47% reported weaker-than-expected psychedelic effects. The same study concluded that SSRI use can weaken psilocybin effects, as described in the PubMed study on attenuation during and after SSRI or SNRI use.

What “weaker” usually means
“Weaker” doesn't just mean fewer visuals. People often mean one or more of the following:
- Less intensity overall
- A shorter or flatter arc
- Less emotional access
- No obvious psychedelic shift at all
That last outcome is where people get into trouble. If someone expects a standard mushroom experience and feels very little, they may assume the dose was too low and redose aggressively. But if receptor sensitivity and adaptation are part of the issue, chasing the effect can make the situation less predictable without guaranteeing the result you wanted.
Reported effects of combining psilocybin with an SSRI
| Potential Outcome | Description | Reported Frequency |
|---|---|---|
| Weaker-than-expected effects | The psychedelic experience feels muted, flatter, or less intense than anticipated | 47% among SSRI reports |
| Typical or stronger effects | Some people do not report a clear blunting effect | Not precisely quantified in the verified data |
Why this matters for expectations
A lot of harm reduction starts with accurate expectations. If someone believes the combination will work normally, they may plan for a deep trip and get a faint, confusing version instead. That can lead to disappointment, compulsive redosing, or sudden decisions about stopping medication before the next attempt.
Practical rule: If you're on Zoloft and considering mushrooms, don't assume “no big interaction” just because the main outcome may be blunting rather than crisis. A weak effect can still push people into unsafe choices.
This is one of the biggest reasons generic advice falls short. “Don't mix” doesn't tell you what many users experience. “It just weakens the trip” isn't enough either, because people then start looking for shortcuts around that blunting.
Understanding the Real Risks Serotonin Syndrome and Beyond
The muted-effect story is important, but it isn't the whole story. Safety still matters, especially because people rarely use substances in perfectly controlled conditions.
What serotonin syndrome is
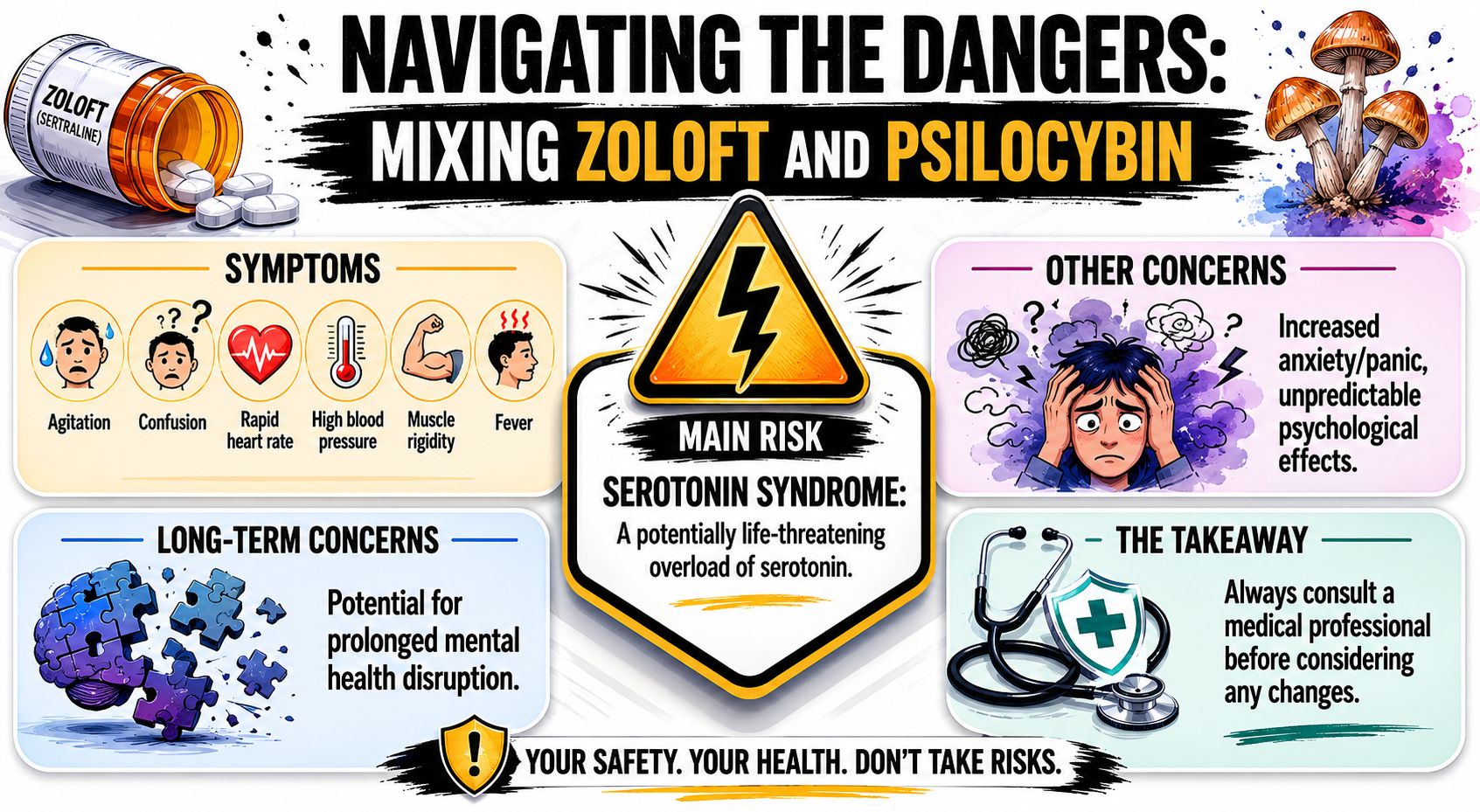
Serotonin syndrome is a toxic overload of serotonin activity. In plain language, the nervous system becomes overstimulated. Symptoms can include agitation, confusion, rapid heart rate, blood pressure changes, muscle rigidity, sweating, and fever. If severe symptoms appear, that is urgent medical territory.
The key point is nuance. Current expert discussion doesn't support the idea that Zoloft plus mushrooms commonly causes serotonin syndrome on its own. The literature instead describes the risk as uncertain and difficult to quantify, with the bigger danger showing up when multiple serotonin-raising substances are stacked together.
Where the red flags really are
Expert reviews note that the highest-risk scenarios involve polypharmacy, such as adding MAOIs, MDMA, certain tramadol-like analgesics, or other serotonergic drugs on top of an SSRI and psychedelic combination, as explained in MIND Foundation's review of psychedelic and antidepressant interactions.
That means the question shouldn't only be “Can I mix Zoloft and mushrooms?” It should also be “What else is in my system?”
Here are the combinations that deserve extra caution:
- Adding MDMA: This pushes serotonin through a different and stronger route.
- Adding MAOIs: These can change breakdown of monoamines and make interactions far less forgiving.
- Mixing with other serotonin-raising meds or supplements: People sometimes overlook how many products can affect the same system.
- Using mushrooms in a chaotic setting while already anxious or unstable: Even without toxicity, psychological distress can become intense and hard to manage.
To understand broader medication overlap, this guide on shrooms and antidepressants gives a wider frame than sertraline alone.
A short video can also help summarize the safety picture before you make any decisions.
Risks that aren't serotonin syndrome
Some of the most immediate harms are psychological and behavioral.
- Panic and confusion: A person expecting warmth or insight may get anxiety, disappointment, or mental turbulence.
- Dose escalation: Chasing a “real trip” can lead to poor judgment.
- Mood destabilization afterward: This matters even more if someone already lives with depression, anxiety, or bipolar-spectrum symptoms.
If you develop a cluster of concerning physical symptoms after mixing substances that affect serotonin, treat that as a medical issue, not something to ride out alone.
Practical Considerations on Timing and Tapering
The most common workaround people consider is simple: stop Zoloft for a few days, then take mushrooms. On paper that sounds tidy. In real life, it can be a bad trade.
Stopping sertraline abruptly can trigger discontinuation symptoms and can also destabilize the mental health condition the medication was helping manage. People often underestimate how rough even a short interruption can feel. The mistake is assuming that because the goal is one psychedelic session, the medication pause is minor.
Why a short break isn't a reliable fix
A Johns Hopkins analysis found that reduced psilocybin effects could persist for up to 3 months after discontinuing an SSRI, which suggests there's no quick, evidence-based washout rule for restoring a full psychedelic effect, as described in the Johns Hopkins analysis of post-discontinuation attenuation.
That finding changes the practical decision. If a short pause may not restore the effect anyway, then the person may be taking withdrawal risk without getting the result they wanted.
The real tapering question
Tapering is a medical process, not a hack.
A supervised taper considers things like your current dose, how long you've been on sertraline, why you're taking it, how you've responded to past dose changes, and whether your mood gets worse when serotonin support is reduced. That's one reason there isn't a universal answer to “How long should I stop Zoloft before mushrooms?” Current evidence doesn't support a clean one-size-fits-all number.
Here are the practical takeaways:
- Don't stop Zoloft abruptly just to make mushrooms work better. That can create a new problem immediately.
- Don't assume a weekend break changes much. The interaction may outlast the period you expected.
- Don't self-test while already struggling. If your baseline mood is unstable, introducing withdrawal plus psychedelics is a poor setup.
- Do treat medication changes as healthcare decisions. They deserve planning, monitoring, and follow-up.
Metro Mush offers adult-use psilocybin products in Southeast Michigan, including dried mushrooms and edibles like OuterSpore Milk Chocolate Bars, Mush Love Chocolate Bars, Rocket Fuel shroom drinks, and Moon Bars. If someone is considering any product while prescribed sertraline, the interaction question should be settled with a clinician first, not by trial and error.
A lot of people ask for the “minimum time off” Zoloft. The more honest answer is that a short pause may be risky, may not solve the blunting problem, and may leave you feeling worse before you even get to the mushroom experience.
The Only Safe Path Forward Is With Your Doctor
At this point, the shape of the issue is clearer. With Zoloft and mushrooms, the likely concern for many people is reduced psychedelic effect, but that doesn't make self-experimentation harmless. The interaction is still pharmacologically complicated, personally variable, and easy to handle badly.
Your doctor isn't just there to say yes or no. They can help you think through the part the internet can't answer for you. Why are you on sertraline? How stable are you right now? What happened the last time your dose changed? Are there other medications, supplements, or substances in the picture? Those details matter more than generic online advice.
If you're interested in a structured clinical model rather than informal use, this overview of what psychedelic therapy involves can help you frame a more informed conversation.
The safest next move is honesty. Tell your prescriber what you're considering. Ask about interaction risk, tapering risk, relapse risk, and what warning signs would make any plan unsafe. If they don't know much about psychedelics, that still doesn't make self-management a better option. It means you may need a clinician with more relevant experience.
Frequently Asked Questions About Zoloft and Mushrooms
Some questions still come up even after people understand the basics. The table below answers the ones that matter most in plain language.
| Question | Answer |
|---|---|
| Can I safely take Zoloft and mushrooms together? | There's no simple “safe for everyone” answer. The interaction appears more likely to blunt the psychedelic effect than to cause a dramatic reaction by itself, but the safety picture gets more concerning if other serotonin-raising substances are involved, or if your mental health is already unstable. |
| Should I stop Zoloft for a few days before taking mushrooms? | That's usually a bad shortcut. Abrupt or unsupervised stopping can cause discontinuation symptoms and mood destabilization, and a brief pause doesn't guarantee the psilocybin effect will return. |
| How do I know when it's a medical emergency? | If someone develops a concerning mix of physical symptoms such as agitation, confusion, rapid heart rate, muscle rigidity, sweating, or fever after combining substances, get medical help right away. Don't try to tough it out alone. |
| Does a weaker trip mean I should take more mushrooms? | Not necessarily. Redosing to overpower SSRI-related blunting can make the experience less predictable and may increase risk without producing the result you want. |
| What's the smartest next step if I'm curious about psilocybin? | Talk with your prescriber before making any change to sertraline. If your interest is therapeutic, ask about supervised options and whether medication changes are appropriate for your situation. |
The headline takeaway is simple. Zoloft and mushrooms is not just a yes-or-no safety question. It's a question about blunted effects, uncertain interaction, medication stability, and how much risk you're taking on by trying to force a certain kind of psychedelic experience.
If you're researching psilocybin carefully and want product information alongside education, Metro Mush publishes guides on topics like antidepressant interactions and psychedelic therapy, while also listing adult-use mushroom products available in the Detroit and Ann Arbor areas.