You might be here because you're curious about psilocybin, but you also take a daily medication and don't want to guess your way into a bad outcome. That's a smart place to start. A lot of people aren't asking, "Will this work?" They're asking, "Will this be safe for me, with my brain, my prescription, and my body?"
That question matters because psilocybin drug interactions aren't all the same. Some combinations mainly blunt the experience. Some can change the physical effects. A smaller group can become dangerous. If you only hear "safe" or "unsafe," you miss the part that helps you make a decision.
This guide takes a harm reduction approach. It's educational, not medical advice, and it isn't a substitute for talking with a doctor or pharmacist who knows your health history. But if you want a clearer mental model of what's happening when psilocybin meets antidepressants, antipsychotics, mood stabilizers, or other substances, this will help you think about it in a calm and practical way.
Navigating Your Journey with Psilocybin and Medications
A common situation looks like this. Someone has been managing depression, anxiety, or another mental health condition with prescribed medication. At the same time, they're interested in psilocybin for insight, relief, curiosity, or a more intentional experience.
That person often runs into two bad kinds of advice. One says every medication mix is automatically catastrophic. The other says medications don't matter and you should just "send it." Neither is responsible.
The question isn't only risk
With psilocybin drug interactions, there are really two separate questions:
- Could this combination be dangerous: Meaning it could raise the chance of a serious medical or psychiatric problem.
- Could this combination change the experience: Meaning it might weaken, flatten, shorten, or otherwise alter what psilocybin feels like.
Those are not the same thing.
If a medication blunts psilocybin, that doesn't automatically mean an emergency. If a medication creates a high-risk interaction, that's a different category entirely. Keeping those categories separate helps you avoid two mistakes at once. Overreacting to lower-risk blunting, and underreacting to combinations that deserve a hard no.
Practical rule: Don't ask only, "Can I mix these?" Ask, "What kind of interaction is this?"
Why people get confused
Part of the confusion comes from the word "block." People say antidepressants "block" mushrooms as if the brain were a light switch. Real life is messier. The same medication can affect the subjective trip, the body's response, and the overall safety picture in different ways.
Another reason is that stopping a prescription isn't simple harm reduction. It can create its own problems, including relapse, withdrawal, or instability. That's why the safest path usually starts with understanding the mechanism, not chasing myths from comment threads.
How Psilocybin Drug Interactions Actually Happen
Psilocybin gets converted in the body into psilocin, which interacts with serotonin-related systems in the brain. The easiest way to understand this is with a lock-and-key model.
Think of certain brain receptors as locks. Think of chemicals as keys. Psilocybin's active form is one of the keys that can fit an important serotonin-related lock, especially the 5-HT2A receptor, which is closely tied to changes in perception, meaning, mood, and sense of self.
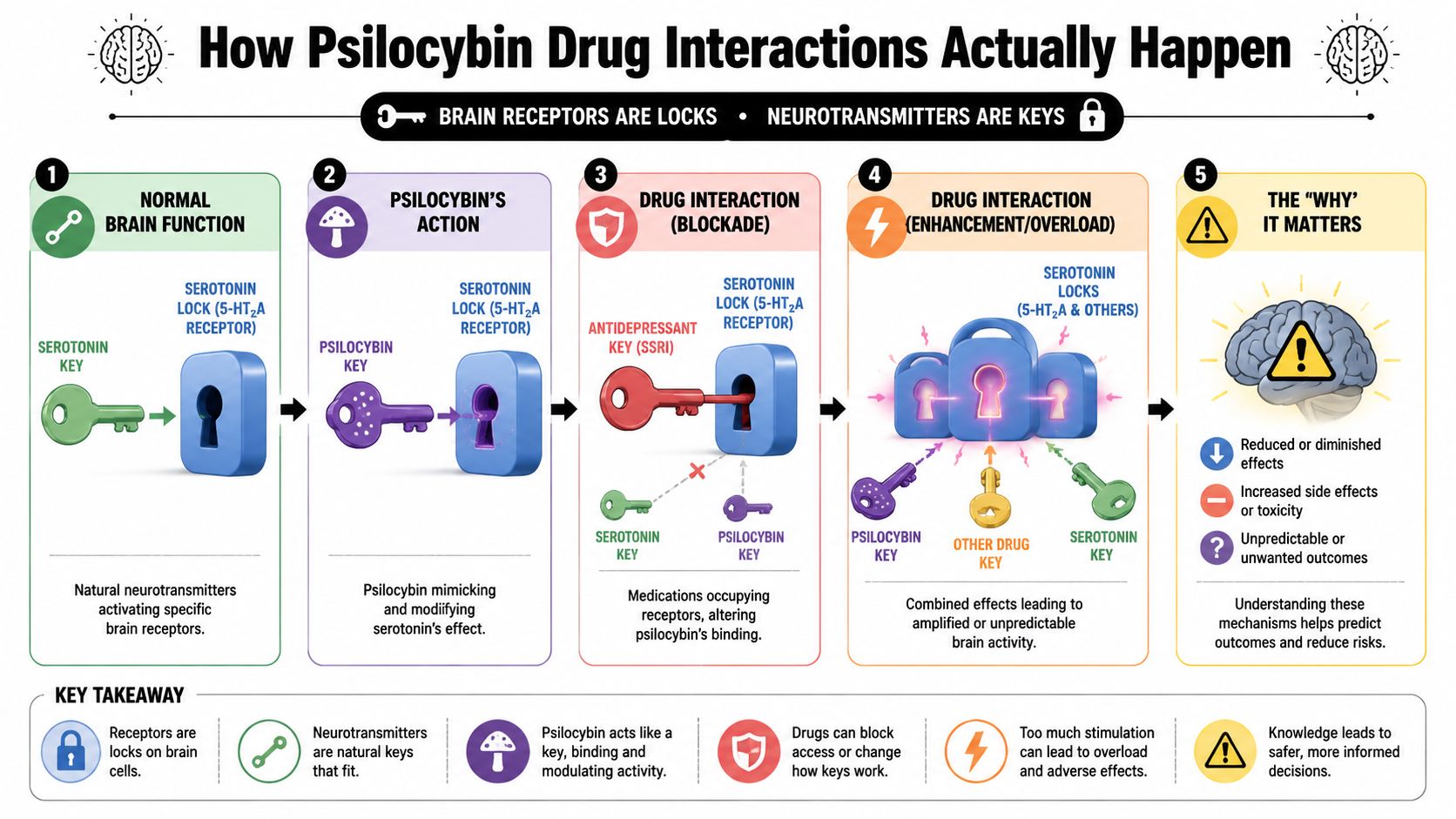
The three main interaction types
Once you picture receptors as locks, most psilocybin drug interactions make more sense. They usually fall into one of these patterns:
Blunting
Another medication changes the lock so psilocybin's key doesn't work as strongly. The result may be a flatter or weaker experience.
Blocking
A medication pushes strongly in the opposite direction, reducing the psychedelic effects more dramatically.
Overload or instability
Multiple substances affect related systems at the same time, creating a more unpredictable picture that can become physically or psychiatrically unsafe.
Why chronic medications can change the response
Some medications don't only compete in the moment. They change the brain's sensitivity over time.
Research describes this with 5-HT2A receptor desensitization and cross-tolerance. Chronic use of drugs like SSRIs can down-regulate these receptors, which means the brain can become less responsive to psilocybin. That reduced responsiveness may persist for up to 3 months after stopping the medication, according to a review discussing receptor desensitization and prolonged washout considerations in this article on psilocybin pharmacology and serotonergic interactions.
That's why two people can take the same amount of psilocybin and report completely different results. One person may feel a full emotional and perceptual shift. Another may feel only mild mood change, body load, or a vague sense that something is trying to happen but never fully arrives.
A simple analogy that helps
If psilocybin is a key, SSRIs often don't "jam the lock" in the dramatic way people imagine. Over time, they can make the lock less responsive. Antipsychotics can act more like a stronger opposing force, making it harder for the key to do much at all.
If you want a broader primer on how psilocybin affects perception and signaling, this overview of psilocybin effects on the brain gives helpful background.
A changed experience isn't always a sign that the product is weak. Sometimes the nervous system is simply responding differently because of another medication.
The Big Question Psilocybin and Antidepressants
You take mushrooms expecting a strong shift in mood, perception, or insight. Instead, the experience feels thinner than expected. Colors may look a little brighter, your body may feel altered, but the deeper psychological effects never fully arrive. For people taking antidepressants, that pattern comes up often, and the main question is usually the same. Is the combination dangerous, or is it more likely to change the experience itself?
For SSRIs and SNRIs, the answer is often about blunting, not necessarily acute danger. That distinction matters. A blunted interaction means psilocybin may feel weaker, flatter, or less immersive. A dangerous interaction means the combination raises the chance of a serious medical event. Those are different categories, and mixing them together creates a lot of confusion.
What researchers have observed
A Johns Hopkins publication based on 611 reports found a 0.47 probability of weaker-than-expected psilocybin effects during SSRI use, with a 95% confidence interval of 0.41 to 0.54, according to the Johns Hopkins publication on attenuation of psilocybin mushroom effects during and after SSRIs/SNRIs.
That finding fits what many people describe in plain language. The mushrooms still do something, but the signal can come through like a dimmer switch was turned down. Visual changes may be lighter. Emotional release may feel harder to reach. The sense of depth or momentum may never build in the usual way.
The same publication reported that reduced sensitivity may continue for up to three months after stopping an SSRI or SNRI. So a brief pause is not a reliable reset, and stopping antidepressants on your own can create withdrawal symptoms or a return of depression and anxiety symptoms that carry their own risks.
Why the experience can change without disappearing
Psilocybin works largely through serotonin signaling, especially at the 5-HT2A receptor. Many antidepressants also affect the serotonin system, but in a different way and over a longer time frame. A useful comparison is volume versus wiring. Psilocybin tries to send a strong signal in the moment. Chronic antidepressant use can change how responsive part of that signaling system is over time.
That helps explain why antidepressants do not always "cancel" psilocybin. In many cases, they appear to reduce intensity rather than fully block the experience. For some people, that means a softer trip. For others, it means frustration, repeated redosing, or assuming the mushrooms were weak when the actual difference may be medication-related.
Blunted effects and therapeutic effects are not the same question
A weaker psychedelic experience does not automatically mean zero benefit. A review examining open clinical questions around psilocybin noted that some patients taking chronic SSRIs still appeared to show antidepressant improvement after psilocybin treatment, as discussed in this review on psilocybin interactions and clinical questions.
That point is easy to miss. Subjective intensity and therapeutic outcome are related, but they are not identical. Someone may have fewer visuals or less ego dissolution and still notice meaningful shifts in mood, perspective, or emotional processing. The reverse can also happen. A strong trip is not a guarantee of lasting benefit.
What this means in practical terms
If you take an SSRI or SNRI, a few outcomes are common:
- The experience may be muted. Effects can feel weaker, delayed, or incomplete.
- The response may be uneven. You might notice body effects or mild perceptual changes without the fuller psychological shift you expected.
- Stopping medication can create its own harm. Any taper should be handled with your prescriber, not improvised around a planned trip.
If antidepressants are your main concern, this guide on shrooms and antidepressants goes deeper into specific medication types and common questions.
A different response does not always mean a dangerous interaction. With antidepressants, it often means the experience may be altered in ways that are hard to predict without medical guidance.
High-Risk Combinations You Must Avoid
A muted trip and a dangerous interaction are different problems. One changes what you feel. The other can raise the chance of a medical or psychiatric emergency.
That distinction matters here.
Lithium and similar mood stabilizer concerns
Lithium is the clearest red-flag combination. Case reports have linked lithium taken alongside classic psychedelics, including psilocybin, with seizures and episodes of mania. The concern is not just that the trip may feel strange or intense. The concern is loss of stability in the brain systems that regulate mood and electrical activity.
A simple way to frame it is this. Psilocybin pushes serotonin signaling in a direction that can be psychologically destabilizing for some people. Lithium affects mood regulation through a different set of brain mechanisms. In a small number of people, that mix appears to create the kind of unpredictability that harm reduction tries to avoid entirely.
If you take lithium, treat psilocybin as a combination that needs direct medical guidance first, not experimentation. Metro Mush's harm reduction approach to substance decisions starts with that question: is the possible benefit worth the worst plausible outcome?
Lamotrigine belongs in a more uncertain category. It does not carry the same level of concern as lithium based on the limited reports available, but it is still a medication that signals a more complex mental health picture. That alone is reason to slow down and get professional input.
Antipsychotics can block effects and complicate the experience
Antipsychotics are often misunderstood. They do not just make psilocybin “safer” by turning it down. Many of them block the same serotonin receptor psilocybin relies on, especially 5-HT2A, so the result can be a flat, incomplete, or cognitively unpleasant experience.
That is a different interaction type from lithium. With antipsychotics, the main pattern is blocking or distorting the effects, not reliably creating a stronger trip. But safety is still part of the picture. If someone takes an antipsychotic because of psychosis, bipolar disorder, or severe mood instability, using psilocybin on top of that can still be destabilizing even if the drug partly blocks the trip.
In other words, this is not a clean cancel-out. It can turn into a confused middle ground where the desired effects are weakened, but the underlying vulnerability is still there.
Other combinations that deserve a very cautious approach
Some pairings do not fit neatly into “blunting” or “blocking.” They add unpredictability.
- MAOIs: These can change how serotonin-related compounds are processed and may make psilocybin's effects harder to predict. The risk is less about a guaranteed outcome and more about losing your ability to estimate dose and intensity.
- Tramadol: This medication has serotonergic effects and can lower seizure threshold. That combination raises concern because the risk profile shifts away from simple trip variation and toward possible medical complications.
- A personal history of mania, psychosis, or seizures: Your own response history matters as much as the drug list. If a substance or medication has pushed you into one of those states before, psilocybin deserves extra caution.
Signs that call for urgent help
Get immediate medical help if someone has:
- Seizure activity: Shaking, collapse, loss of consciousness, or a period of unresponsiveness
- Extreme agitation or confusion: They cannot be calmed, cannot recognize familiar people, or become impossible to redirect
- Severe physical distress: Chest pain, trouble breathing, rigid muscles, dangerous overheating, or persistent vomiting
- Escalating mania or psychosis: No sleep, racing thoughts, grandiosity, panic, paranoia, or behavior that is becoming unsafe
The safest way to judge a combination is by its worst realistic outcome, not by a reassuring story from a forum.
Psilocybin Drug Interactions at a Glance
Sometimes you don't need a long explanation first. You need a quick scan of the category you're dealing with.
Psilocybin Interaction Summary by Drug Class
| Drug Class | Risk Level | Interaction Type & Notes |
|---|---|---|
| SSRIs and SNRIs | Moderate | Blunting. Often reported to weaken expected effects. The experience may feel flatter or less visual. Stopping medication without supervision can carry its own risks. |
| MAOIs | High | Potentially unpredictable. This combination can alter intensity and safety in ways that are hard to forecast. Avoid unsupervised use. |
| Lithium | High | Dangerous. Research has linked this category to severe adverse effects including seizures and manic episodes. |
| Antipsychotics | High | Blocking plus potential harm. These can strongly dampen the psychedelic experience and may contribute to a cognitively unpleasant or destabilizing response. |
| Benzodiazepines | Moderate | Blunting or trip interruption. People sometimes use them to calm overwhelming experiences, but combining substances without planning can muddy the outcome. |
| Stimulants such as Adderall | Moderate to high | Activation and unpredictability. May increase tension, overstimulation, or cardiovascular strain in some people. |
| Cannabis | Variable | Unpredictable enhancement. For some, it deepens the experience. For others, it increases confusion, anxiety, or dissociation. |
| Alcohol | Moderate to high | Reduced clarity and judgment. Can make it harder to assess what you're feeling and respond well if something starts going wrong. |
How to use this table
Treat the table as a first filter, not a final answer.
If your medication falls into a high-risk category, don't use the table to justify trying it anyway. If it falls into a moderate or variable category, the next step is to look at your exact medication, your dose, your health history, and whether a prescribing professional can guide you.
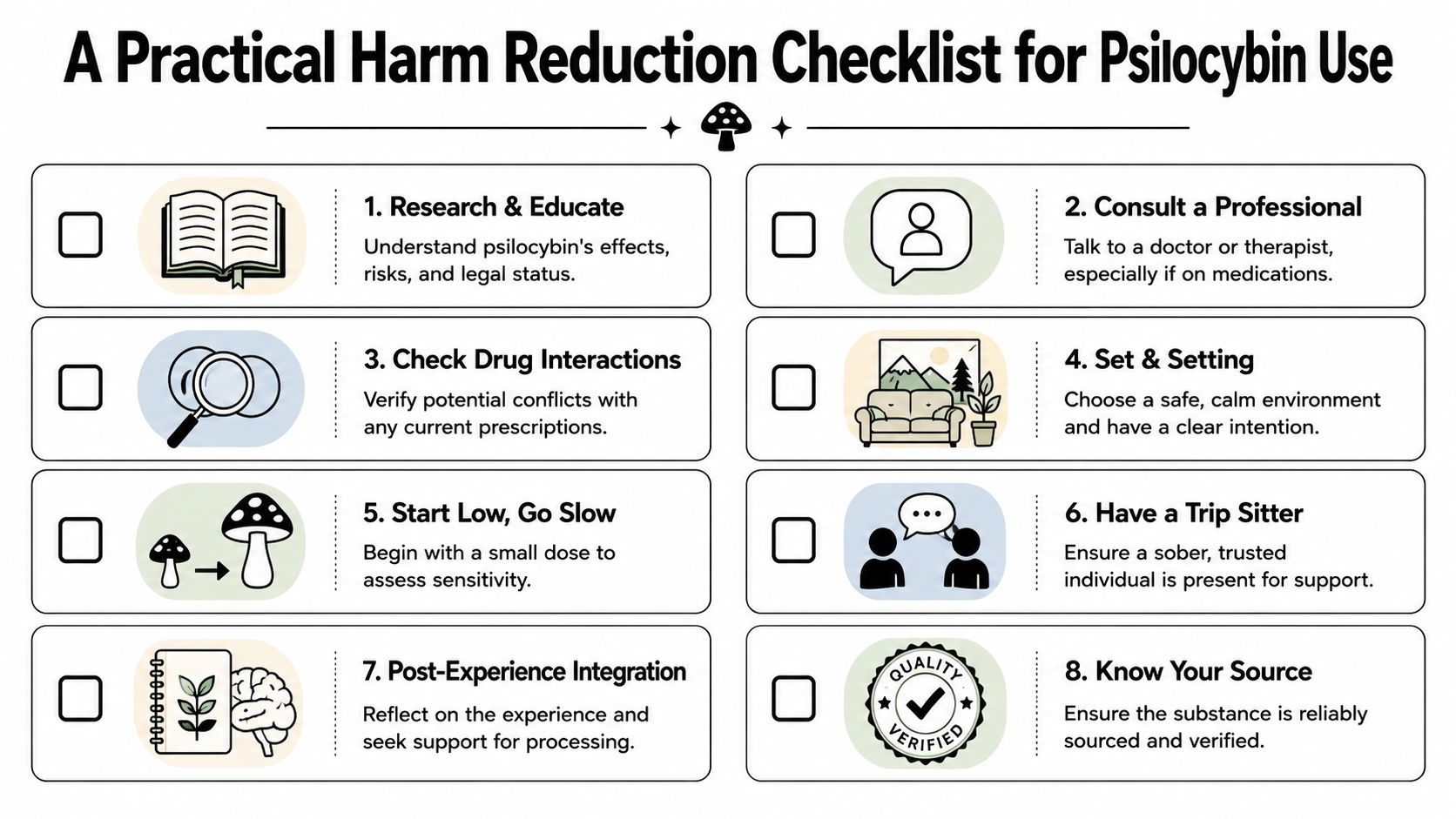
A Practical Harm Reduction Checklist
Good harm reduction is boring in the best way. It replaces guessing with preparation.
Start with the medication list
Before thinking about dose, write down everything you're taking. That includes prescriptions, over-the-counter drugs, supplements, and anything used "only sometimes."
Use this simple sequence:
- Name the exact substance: Not just "an antidepressant," but the specific medication.
- Note how often you take it: Daily, as needed, recently stopped, or tapering.
- Check whether the interaction is blunting or dangerous: Those are different decisions.
- Bring that list to a doctor or pharmacist: Especially if you take psychiatric medication.
If you want a broader safety framework, this harm reduction guide is worth reading alongside this one.
Build the experience around safety
The best checklist isn't only pharmacology. It's also planning.
- Consult a professional: If you're on an SSRI, SNRI, antipsychotic, lithium, lamotrigine, or a complex medication regimen, get individualized guidance before doing anything.
- Respect washout periods: Some medications keep affecting receptor sensitivity after the last dose. A short break doesn't always mean your brain has returned to baseline.
- Start low and go slow: If there is any uncertainty, lower-intensity experimentation is safer than jumping straight to a big dose.
- Choose a calm setting: Comfortable space, minimal obligations, no driving, no decision-heavy tasks.
- Have a sober sitter: Pick someone grounded, nonjudgmental, and willing to stay present if your experience gets confusing.
A visual reminder can help when you're planning with other people.
Know what to do if things feel off
It's easier to make a good decision before the experience starts than in the middle of it.
- If the effects are much weaker than expected: Don't stack more immediately out of frustration. Delayed or blunted experiences can tempt people into redosing too fast.
- If anxiety spikes: Reduce stimulation. Lower lights, reduce noise, breathe slowly, and let the sitter do the talking.
- If there are signs of physical danger or psychiatric emergency: Stop treating it like a rough trip and get medical help.
Quick check: If you're relying on guesswork about your prescription, you're not ready yet.
Where to Go for Support and Guidance
The most protective move you can make is still the simplest one. Talk to a qualified healthcare professional who can look at your specific medication, diagnosis, and history. Online guides can teach patterns, but they can't tell you what your own nervous system will do.
That matters most if you have a history of bipolar symptoms, mania, psychosis, seizures, or severe panic. It also matters if you've recently changed medications, started tapering, or are taking more than one psychiatric drug at the same time.
When to seek immediate help
Don't wait it out at home if someone is having:
- A seizure or loss of consciousness
- Chest pain or trouble breathing
- Extreme confusion, violent agitation, or inability to recognize reality
- A manic or psychotic state that is intensifying
- Dangerous overheating or signs of severe physical distress
- Thoughts or actions suggesting self-harm or harm to others
In those situations, emergency care matters more than privacy or embarrassment.
Local support and practical questions
For product questions in Southeast Michigan, Metro Mush offers direct text support for the Detroit Metro at 734-691-6122 and the Ann Arbor Metro at 734-280-2868. If you prefer community updates and peer connection, their Discord is another place people can stay in touch and hear about new drops and promotions.
The right support depends on the question. Medical safety questions belong with a clinician or pharmacist. Product and menu questions belong with the shop. Emotional support during planning belongs with trusted, sober, informed people.
A careful decision can still be a confident one.
If you're an adult in Southeast Michigan looking for a reliable local option, Metro Mush offers a curated menu of psilocybin products, including dried mushrooms, chocolate bars, drinks, and other approachable formats. You can browse the menu online, check locations, and place orders by text for Detroit Metro or Ann Arbor Metro delivery and pickup support.