You may be in a very ordinary situation. You take an SSRI for depression or anxiety, you've heard people talk about psilocybin, and now you're trying to sort out one basic question. Can these two things mix safely, and if not, how long do you need to wait?
That confusion makes sense. A lot of advice about SSRI and psychedelics is too simple to be useful. One source says “just stop for a few days.” Another says “never combine them.” A better answer is more nuanced. There are really two different questions people often mash together: acute safety right now, and whether your brain may still respond differently even after the medication is out of your system.
This guide takes a harm reduction approach. It won't tell you what to do with your body or your treatment. It will help you understand what's known, what's uncertain, and where people often get tripped up.
The Common Crossroads of Antidepressants and Psychedelics
A lot of people assume they're in a rare gray area if they take antidepressants and are curious about psychedelics. They're not. In the United States, 13.2% of adults reported antidepressant use in the past 30 days during 2015 to 2018, and use was 17.7% for women, according to the CDC data brief on antidepressant use.
That matters for one simple reason. If antidepressant use is this common, then a large number of adults exploring psilocybin are also navigating the same medication question.
Why this isn't a fringe issue
People don't usually arrive here because they're careless. Many are trying to balance mental health treatment, curiosity about psychedelic therapy, and practical safety. Some are wondering whether psilocybin might help them. Others are already experienced with mushrooms and then start an SSRI later. Some want to know whether microdosing changes the equation.
All of those questions are reasonable.
Many adults aren't choosing between “medication people” and “psychedelic people.” They're trying to make sense of both at once.
The problem is that online advice often collapses everything into one sentence. “SSRIs block mushrooms.” Or “wash out for a week.” Or “it's dangerous.” None of those statements is complete on its own.
The more useful frame
Think of this topic as having three layers:
- Current medication effects: If you're still taking an SSRI, your brain's serotonin system is already being influenced every day.
- Immediate interaction risk: Taking a psychedelic while on an SSRI raises a safety question because both affect serotonin signaling.
- Lingering changes after stopping: Even if the drug itself has cleared, your brain may not have snapped right back to baseline.
That last point is where many guides fall short. They focus only on the medicine leaving your bloodstream, as if that ends the story. It often doesn't.
If you remember one thing from this article, make it this: with SSRI and psychedelics, the key issue isn't just “Is the pill out of my body?” It's also “How is my brain responding now?”
How SSRIs and Psychedelics Affect Your Brain
The easiest way to understand this interaction is to stop thinking in terms of labels and start thinking in terms of traffic.
Your serotonin system is like a busy road network. Serotonin is part of the traffic. Receptors are the exits and on-ramps that control where signals go. SSRIs and classic psychedelics both affect this system, but they do it in different ways.
What SSRIs do
SSRIs increase serotonin signaling by blocking reuptake. In plain language, they make serotonin stick around longer instead of being pulled back in quickly. It's a bit like slowing the cleanup crew so more signal stays active in the system.
That doesn't mean SSRIs “add happiness chemicals” in a simple way. It means they change the background conditions under which serotonin signaling happens.
What psychedelics do
Classic psychedelics such as psilocybin act through serotonin pathways too, especially at the 5-HT2A receptor. If SSRIs change the traffic pattern, psychedelics are more like a vehicle that takes a very specific exit and then changes what happens downstream.
This is why the combo is complicated. These substances aren't acting in separate rooms. They're operating in the same building.
If you want a deeper primer on the biology behind psilocybin itself, Metro Mush has a useful overview of psilocybin effects on the brain.
Why the combination can feel unpredictable
People often get confused because they expect one of two clean outcomes. Either “nothing happens” or “it's dangerous.” Real life is messier.
A more accurate mental model looks like this:
| Situation | What's happening in the serotonin system | What that can mean |
|---|---|---|
| No SSRI present | Baseline serotonin handling | Psychedelic effects may unfold more typically |
| On an SSRI | Serotonin signaling is already being altered daily | Psychedelic effects may feel muted or different |
| Recently stopped an SSRI | Drug may be leaving, but system may still be adapting | Safety and effect intensity may not reset on the same timeline |
Practical rule: Don't reduce this topic to a single yes-or-no question. Ask two questions instead. “What is the safety risk?” and “What is my likely response?”
That split matters. Acute safety and subjective effect aren't the same thing. A person may avoid a severe reaction and still find the psychedelic experience unexpectedly flat, emotionally muted, or inconsistent.
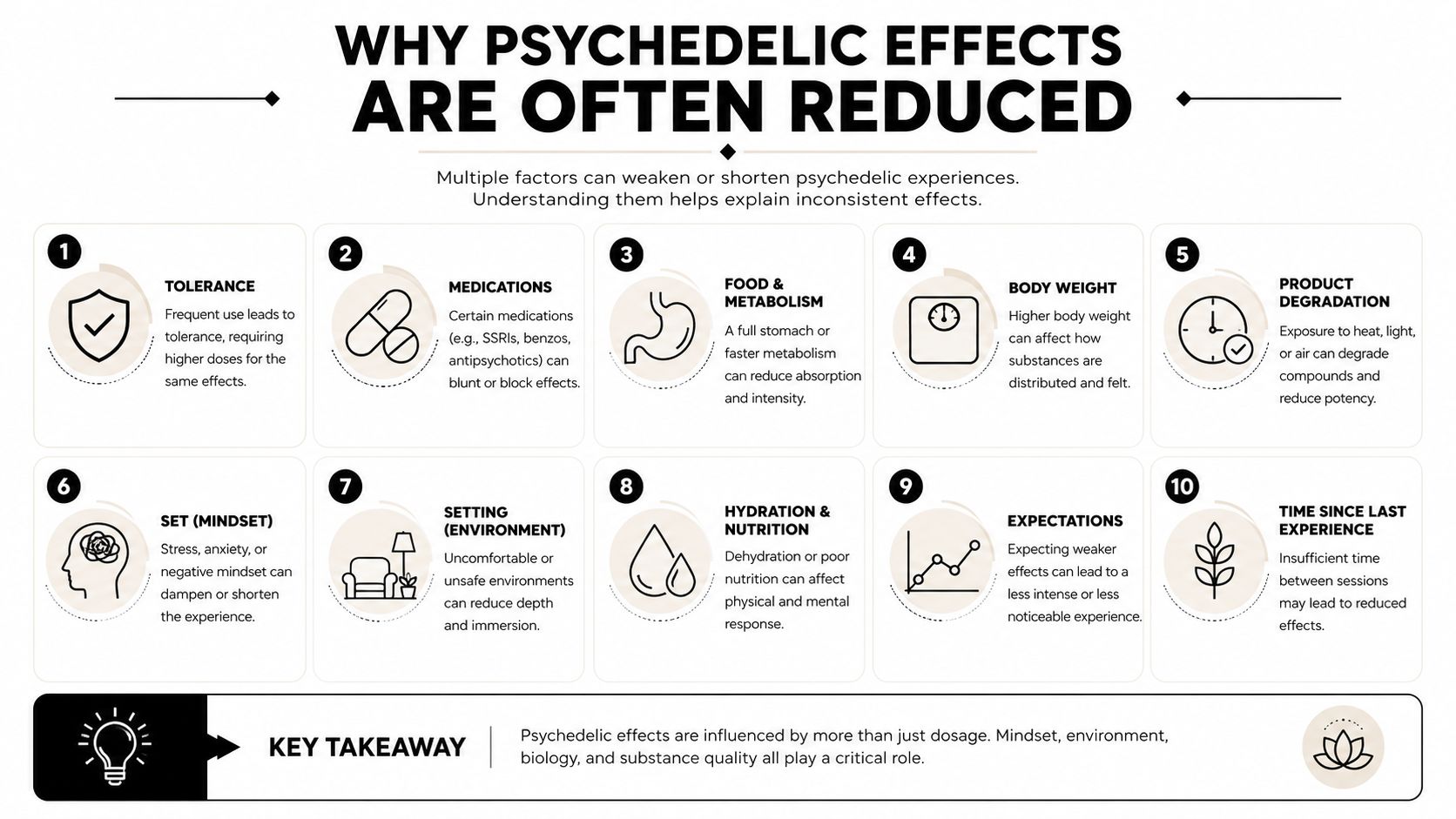
Why Psychedelic Effects Are Often Reduced
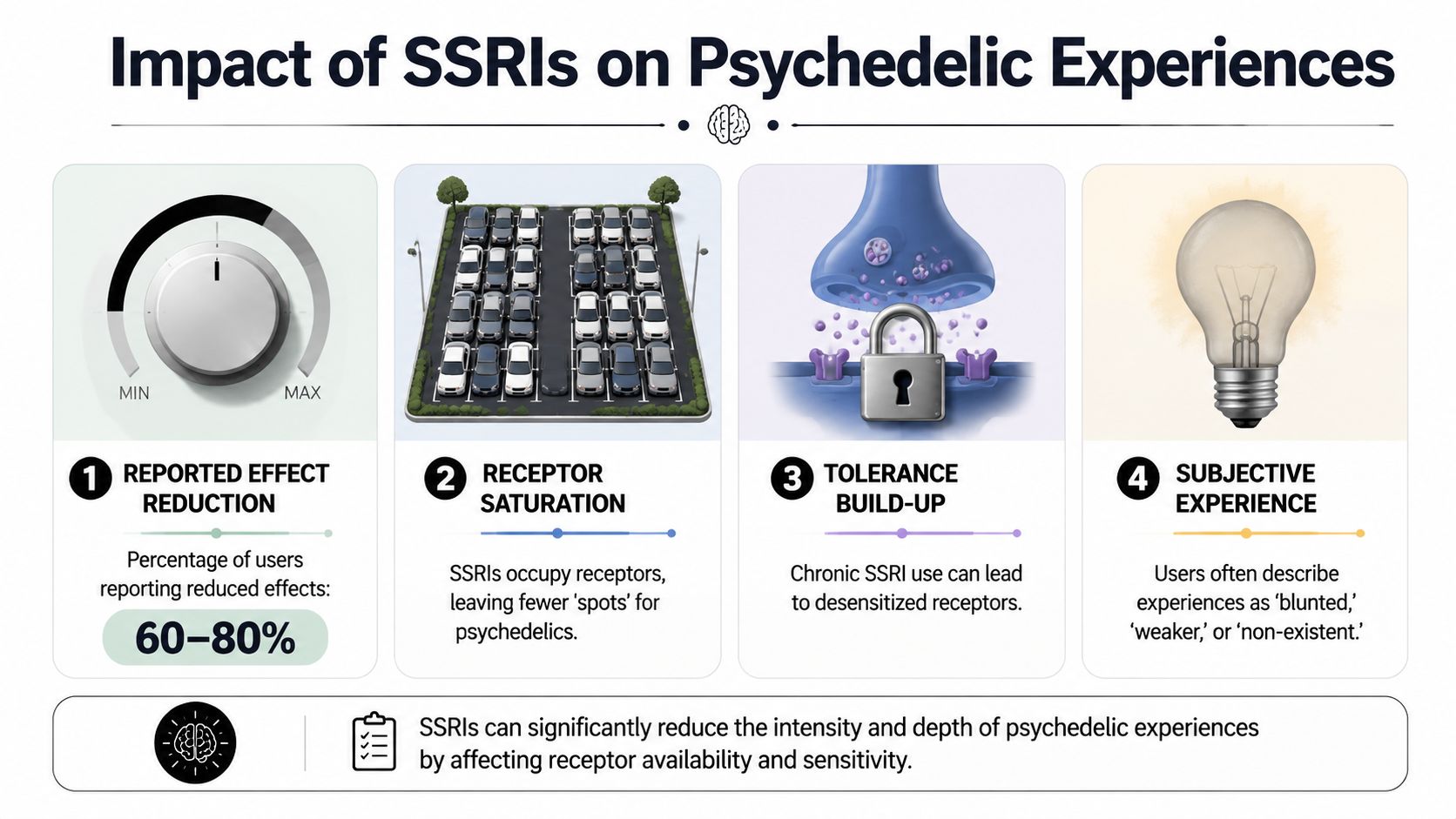
The most common real-world report isn't total cancellation. It's attenuation, which means the psychedelic experience may still happen, but with less depth in certain areas.
That lines up with human data. In a study of psychedelic users, people not taking serotonergic reuptake inhibitors reported stronger acute effects than those taking them. Compared with SRI-positive participants, the SRI-negative group reported 18.2% stronger mystical experiences, 50.9% stronger challenging experiences, and 31.9% stronger emotional-breakthrough experiences, while visual alterations were not significantly different, according to the Johns Hopkins linked study in PMC.
Why the emotional side is hit harder
A lot of people think a “strong trip” just means strong visuals. That's only part of it. For many users, the most meaningful parts are emotional release, insight, and the sense that long-stuck feelings finally moved.
Chronic SSRI exposure appears to blunt those affective dimensions more than the visual ones. A simple analogy helps. If your emotional volume knob has been turned down over time, psilocybin may still switch on the lights, but the music may come through softer.
That doesn't mean the experience is worthless. It means expectations need to be realistic.
Why this happens biologically
One likely explanation is receptor down-regulation or desensitization. When the brain is exposed to altered serotonin signaling over time, it adapts. It's trying to keep things balanced.
Imagine living next to train tracks. At first every train grabs your attention. After a while, your nervous system adjusts. In a similar way, chronic SSRI or SRI exposure may leave some serotonin-related signaling pathways less responsive.
This helps explain why a psychedelic may not feel “blocked” across the board. Instead, specific parts of the experience can lose intensity.
A short visual explanation can help if you're trying to connect the science with lived experience.
What people often misread
Here are the common interpretation errors:
- “If I still see visuals, the SSRI isn't affecting anything.” Visual changes can still occur even when emotional and mystical aspects are reduced.
- “If the experience feels weak, I should keep redosing.” That can create new safety problems without guaranteeing the experience you wanted.
- “A blunted trip means I did something wrong.” It may reflect a predictable medication interaction.
A dampened response isn't necessarily a failed psychedelic. It may be your current neurochemistry doing exactly what pharmacology would predict.
For someone considering psilocybin while on an SSRI, this is one of the most important expectation-setting points. The question often isn't whether something will happen. It's which parts of the experience may happen less strongly.
Understanding the Risk of Serotonin Syndrome
The most serious concern in discussions of SSRI and psychedelics is serotonin syndrome, also called serotonin toxicity. This refers to a state where serotonin activity becomes excessive and starts causing dangerous symptoms.
From a pharmacology standpoint, the concern is straightforward. SSRIs affect serotonin signaling, and classic psychedelics also act through serotonergic pathways, including 5-HT2A activity. Because of that overlap, expert reviews treat the combination as a potential serotonin-toxicity risk and recommend caution. The MIND Foundation review on psychedelic antidepressant interactions notes that tapering antidepressants before psychedelic use and waiting at least five weeks after SSRI discontinuation appears safer.

What serotonin syndrome actually looks like
This isn't just “feeling weird” or “having a bad trip.” It's a medical problem involving overstimulation.
Symptoms can include:
- Early warning signs: agitation, restlessness, sweating, shivering, diarrhea
- Escalating signs: rapid heart rate, muscle rigidity, tremor, confusion
- Emergency signs: high fever, seizures, severe instability
If someone has severe symptoms after combining serotonergic substances, that's not a “sleep it off” situation. It calls for urgent medical care.
Why the advice sounds cautious even when data are limited
This part confuses many readers. They hear that severe cases from this exact combination aren't clearly established across all compounds, and then conclude there's no meaningful risk.
That's the wrong takeaway.
A lack of definitive all-compound data is not the same as proof of safety. Harm reduction advice often works from mechanism plus caution, especially when the downside is serious. If two substances push on the same serotonin system, clinicians and pharmacology reviewers tend to prefer distance between them.
For readers looking into specific pairings, Metro Mush also has a focused overview on Zoloft and mushrooms.
The practical takeaway
Think about serotonin syndrome like overheating an engine. You don't need your car to catch fire before the warning matters. If you know two factors can raise heat in the same system, the responsible move is to lower stress on that system.
If you're mixing uncertainty with a potential medical emergency, the safest move is to involve a clinician before you involve a psychedelic.
That doesn't mean panic is warranted. It means shortcuts aren't.
The Complicated Question of Washout Periods
“Washout” sounds neat. Stop the SSRI, wait a fixed number of days, and then your brain is ready. In practice, that's too simple.
The first reason is drug clearance. Different SSRIs leave the body at different speeds. The second reason is more important for many people. Your brain's response may remain altered even after the medicine itself is largely gone.
According to Oregon's antidepressant and psychedelics interaction chart, public guidance is inconsistent. A five-week wait is often cited for safety, especially because fluoxetine has a longer half-life, but Johns Hopkins findings also suggest reduced psilocybin response may persist for up to 3 months after stopping SSRIs or SNRIs.
Clearance and response are not the same thing
Many online guides miss the mark here.
A medication can be mostly cleared from the bloodstream while the nervous system is still adapting. Think of moving furniture out of a room. The room is empty. That doesn't mean the carpet springs back immediately.
So when someone asks, “How many days off meds is enough?” the honest answer is often, “Enough for what?”
- Enough to reduce acute interaction risk
- Enough to avoid a muted experience
- Enough to stabilize mood during the taper
Those are related questions, but they aren't identical.
Estimated half-lives of common SSRIs
The exact timeline depends on the medication, the person, and the taper plan. This table is qualitative because one-size-fits-all precision can be misleading.
| SSRI (Brand Name) | Average Half-Life | Estimated Time for Full Washout |
|---|---|---|
| Fluoxetine (Prozac) | Longer half-life | Longer washout than many other SSRIs |
| Sertraline (Zoloft) | Shorter than fluoxetine | Often shorter than fluoxetine, but still individual |
| Escitalopram (Lexapro) | Intermediate | Varies by person and taper plan |
| Paroxetine (Paxil) | Relatively shorter | Clearance may occur sooner, but withdrawal can still be difficult |
| Citalopram (Celexa) | Intermediate | Individualized timing is still needed |
A better way to think about washout
Instead of chasing a universal countdown, use a layered framework:
- Medical taper first. Never stop an SSRI abruptly just to create a psychedelic window.
- Safety window second. A conservative waiting period matters because residual serotonergic effects may persist.
- Response window third. Even after the safety issue improves, the psychedelic may still feel dampened for longer.
That's why “five weeks” and “up to three months” don't conflict. They're answering different parts of the same question.
How to Discuss Psychedelics With Your Doctor
A lot of adults avoid this conversation because they expect judgment. Some worry their doctor will dismiss them. Others worry the conversation will go into their chart in a way that feels uncomfortable.
Still, this is one of the smartest conversations you can have.
Recent analyses suggest that combining antidepressants and psychedelics is generally tolerable across the available literature, but the evidence base is still evolving, and clinicians can help with tapering and individual risk assessment, as described in the JAMA Network Open meta-analysis and review context.
What to say
You don't need to ask for permission in a vague or apologetic way. Be direct, calm, and health-focused.
Try language like this:
“I'm taking an SSRI for my mental health, and I'm also researching psilocybin. I don't want to stop anything abruptly or combine things unsafely. Can we talk through tapering, timing, and risks?”
That framing does three useful things. It shows you're not acting impulsively, it signals that safety matters to you, and it gives the clinician a concrete problem to help solve.
Questions worth bringing in writing
A short list helps keep the appointment productive:
- “What are the risks of stopping this medication too quickly for me?”
- “If tapering is appropriate, what schedule would you recommend?”
- “How would we monitor mood changes or withdrawal symptoms?”
- “How long after discontinuation would you consider the acute interaction risk lower?”
- “What signs would mean I should pause the plan and contact you?”
If your doctor is unfamiliar with psychedelics
That can happen. Keep the discussion anchored in medication safety rather than trying to turn the visit into a debate about psychedelic policy or culture.
You're not asking them to endorse a lifestyle. You're asking them to help you reduce avoidable harm.
If you work with a psychiatrist, primary care physician, therapist, or psychiatric nurse practitioner, each may contribute something different. The prescriber usually guides the taper. A therapist may help track mood and expectations during the transition.
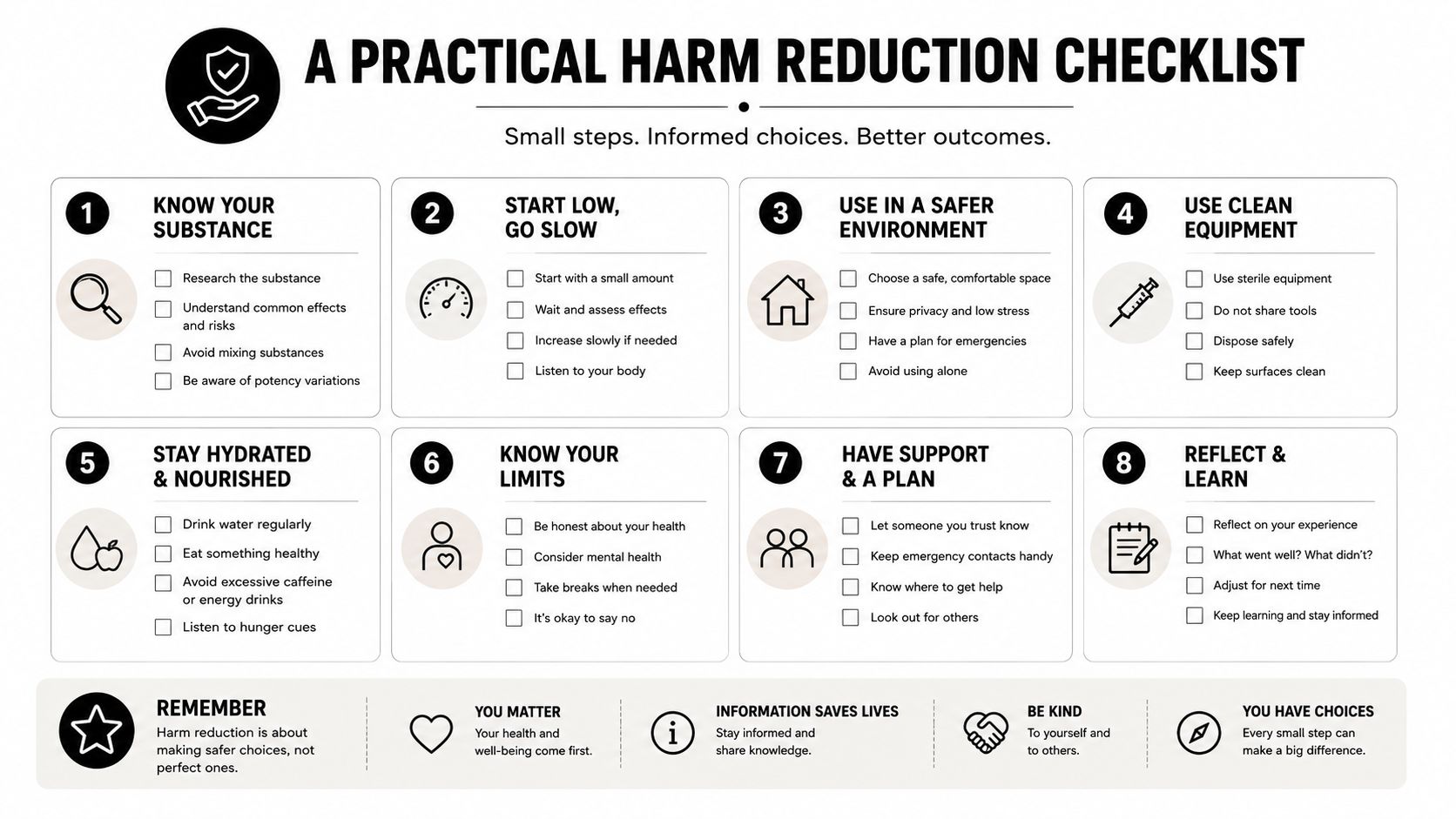
A Practical Harm Reduction Checklist
By the time people look up SSRI and psychedelics, they usually want a clean answer. The safer answer is a checklist. This topic has too many moving parts for a slogan.
Use this list before you change medication, before you plan a session, and before you assume a washout solved everything.
The checklist
Don't stop an SSRI abruptly. Withdrawal, rebound symptoms, and mood destabilization can create more immediate problems than the psychedelic question you're trying to solve.
Separate safety from effect expectations. A waiting period may reduce acute interaction concerns, but it may not fully restore the depth of response you expect.
Assume your first experience may feel different. If you've used psychedelics before without SSRIs, don't expect the same emotional range or insight profile right away.
Avoid stacking substances. Adding other serotonergic or stimulating drugs increases complexity fast. Keep the picture as simple as possible.
Use a sober support person. A trusted sitter helps with observation, emotional grounding, and knowing when a medical issue may be more than anxiety.
Know the warning signs that need help. Agitation, sweating, tremor, confusion, muscle rigidity, high fever, and seizures aren't things to reason away.
Choose setting carefully. A low-stimulation environment, hydration, rest, and a clear plan reduce unnecessary stress if the experience becomes confusing or physically uncomfortable.
Review preparation basics. Metro Mush has a practical guide on how to avoid bad trips on psilocybin that's useful for planning set, setting, and support.
The bottom line
The most responsible framework is simple. Respect the acute serotonin risk, respect the lingering dampening effect, and respect the fact that your mental health treatment shouldn't be yanked around casually for the sake of one experience.
People often want a deadline. “After X days, am I good?” A safer question is, “Have I reduced the medical risk, stabilized my mood, and given my brain enough time to respond more normally?”
If the answer is uncertain, slow down.
If you're an adult in the Detroit or Ann Arbor area looking for straightforward psilocybin education, product information, and local access updates, Metro Mush offers resources designed to help you make informed decisions.